
Updated October 22, 2023
A Vermont advance directive for health care is an estate planning document that lets a person choose a medical agent, select end-of-life wishes, and organ donations. The form can be downloaded and completed on a do-it-yourself basis and after signing may be used in accordance with State law.
Advance Directive Includes
- Part I: Appointment of my Health Care Agent;
- Part II: Others who may be involved in my care;
- Part III: Statement of Values and Goals;
- Part IV: End of Life Wishes;
- Part V: Other Treatment Wishes;
- Part VI: Waiver of Right to Request or Object to Treatment;
- Part VII: Organ and Tissue Donation;
- Part VIII: Disposition of My Body after Death; and
- Part: IX: Signature and Witnesses.
Table of Contents |
Laws
Statute – Title 18, Chapter 231 (Advance Directives For Health Care And Disposition Of Remains)
Signing Requirements (18 V.S.A. § 9703) – At least two (2) witnesses who are 18 years of age or older.
State Definition (18 V.S.A. § 9701(1)) – “Advance directive” means a written record executed pursuant to section 9703 of this title, which may include the appointment of an agent, identification of a preferred primary care clinician, instructions on health care desires or treatment goals, an anatomical gift, disposition of remains, and funeral goods and services. The term includes documents designated under prior law as a durable power of attorney for health care or a terminal care document.
Versions (5)
- Catholic Advance Directive
- Vermont Dept. of Health
- HealthVermont.org (long-form)
- HealthVermont.org (short-form)
- University of Vermont
Download: PDF

Download: PDF

Download: PDF
 HealthVermont.org (short-form)
HealthVermont.org (short-form)
Download: PDF

Download: PDF
Registry
After the advance directive is complete, it may be registered with the State by using the following steps:
Step 1 – Complete the Registration Form.
Step 2 – Attach a copy of the completed advance directive.
Step 3 – Send to the registry by mail or fax to:
Vermont Advance Directive Registry (VADR)
PO Box 2789
Westfield, NJ 07091-2789
Fax: 908-654-1919
How to Write
Download: PDF
Personal Information
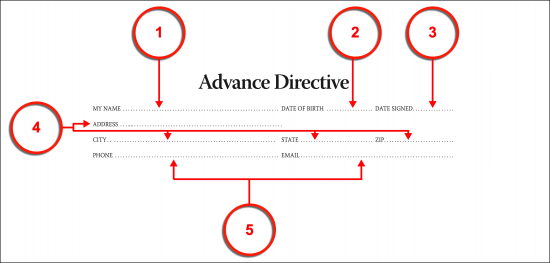
(1) Name. Your name should be displayed at the beginning of this document as the Vermont Patient (sometimes referred to as the Principal or Declarant) issuing this form. In addition to your name, you must supply the supporting information this area expects.
(2) Date Of Birth. Your birth date should be presented.
(3) Date Of Document. The filing date for this paperwork is expected since this will inform Reviewers as to how current the appointment or treatment declarations you are making.
(4) Vermont Patient’s Complete Address.
(5) Phone And Email Address Of Vermont Patient.
Part 1: My Health Care Agent
Article 1
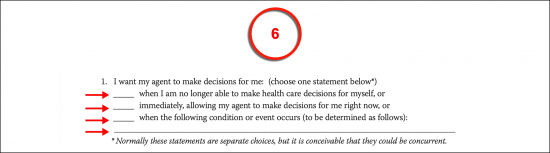
(6) Vermont Health Care Agent Start Date. While the appointment being made is effective once you sign this form, the first calendar date when the Vermont Health Care Agent (or Medical Attorney-in-Fact) is able to access the principal authority this document grants over your medical information and treatment should be defined. You can set this date by providing your initials to one of the statements made on this topic. Initial the appropriate option to indicate you wish your Vermont Medical Attorney-in-Fact to access your principal authority only when you have become unable to make or convey your health care decisions, immediately regardless of your medical condition, or only when prompted by a medical event that you define in the space provided. You may choose one or more of these options as desired, however, make sure you are clear in any prompting event you discuss.
Article 2
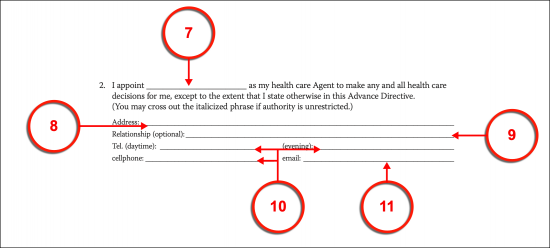
(7) Name Of Vermont Medical Attorney-in-Fact. Furnish the complete name of the Vermont Medical Attorney-in-Fact or Health Care Agent to the declaration made by Article 2.
(8) Vermont Medical Attorney-in-Fact Address. Continue through the second article with the residential address of the Vermont Health Care Agent.
(9) Relationship between Vermont Agent And Principal.
(10) Vermont Attorney-in-Fact Contact Number.
(11) E-Mail Address.
Article 3
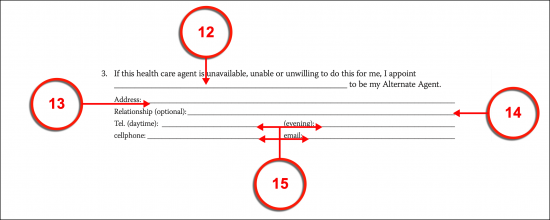
(12) Alternate Agent In Vermont. The Alternate Vermont Health Care Agent appointment available in this section allows you to handle the potential inability or ineffectiveness of the Vermont Medical Attorney-in-Fact that you named above. After all, there is always the possibility that he or she will not be capable of living up to this appointment for a variety of reasons. He or she may be out of the country, may be incapacitated, or may have a significant life challenge that simply doesn’t allow for the time and dedication needed to safeguard your medical preferences when you are completely reliant on his or her representation. You can take an important step in replacing the Vermont Medical Attorney-in-Fact before such a scenario plays out by simply designating an Alternate Health Care Agent to be held in reserve. Therefore, the principal powers the Vermont Medical Attorney-in-Fact will only (automatically) transfer to your Alternate Vermont Health Care Agent should the Attorney-in-Fact fail in his or her appointment for any reason. Take advantage of this safety net by recording the name of someone who you believe would be able to step into this role if needed.
(13) Address Of Alternate Vermont Health Care Agent.
(14) Relationship.
(15) Telephone Numbers And Email Address Of Vermont Agent.
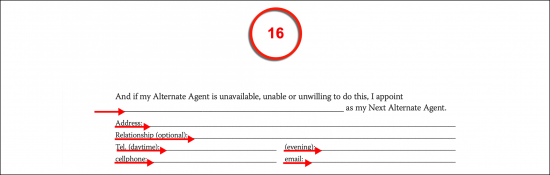
(16) Designation Of Next Alternate Agent. A Second Alternate Vermont Health Care Agent can be designated to automatically receive the principal authority to make medical decisions for you when you are incapacitated by documenting this Party’s name, address, the relationship he or she has with you, and every contact telephone number needed to reach him or her. This Agent will only take over the Vermont Medical Attorney-in-Fact role (and have the power to do so) if both your previous Agents are ineffective.
Article 4
(17) Appointment Of Vermont Co-Agents. If you wish more than one Vermont Medical Attorney-in-Fact to present your treatment decisions or decide when you are unable to, then you must confirm this intention with your initials. It should be noted that the Vermont Health Care Agent will receive the principal authority to decide on your treatment at the same time the Vermont Medical Attorney-in-Fact will. The next portion of this document will allow you to either appoint him or her at a different time as well as indicate how you expect the Vermont Medical Attorney-in-Fact to interact and work with these Co-Agents. This is an optional designation so if you do not intend to name any Co-Agents, leave this statement unattended,

Article 5
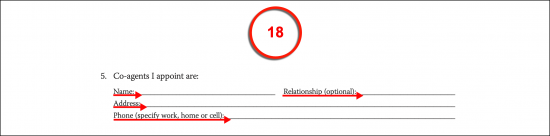
(18) Identify Each Co-Agent. As mentioned, you may appoint as many Co-Agents as you like. This document provides the room to present the name, relationship, address, and contact phone numbers for three Co-Agents. If more room is needed, then you must continue on a labeled attachment. If you wish the Co-Agent’s to have different levels of authority, then list them in order of the Co-Agent with the highest authority to the one with the least and make sure to document this intention within the content of this appointment.
Article 6
(19) Co-Agent Behavior. Since the Co-Agents named will be given the principal powers this document appoints to the Vermont Medical Attorney-in-Fact at the same time, some clarification will be needed to define how these Health Care Agents interact. Article 6 allows you to define health care decisions and actions to be engaged only when all Co-Agents agree to the treatment proposals, the majority of Co-Agents are in agreement, or by the first Agent to be contacted. You may initial one of these statements and/or provide additional instructions.
Article 7
(20) Other Instructions On Co-Agents. You may provide further instructions or conditions on how Co-Agents may decide on your health care treatment. For instance, you may intend to prioritize their decision-making power by naming only one Health Care Agent to have the final say on your treatment and be able to delegate to the other Co-Agents.
(21) Vermont Patient Information.

Part 2 Others Who Are Or May Become Involved In My Care
(22) My Doctor Or Other Health Care Clinician. Produce the name, phone number, and address of your Primary Physician and one other Physician who would be familiar with your medical history. This will enable Vermont Medical Staff to gain information regarding your medical condition in a timely manner.
(23) Other Medical Consultants. Document the name and contact information of any Party or Entity you wish your Vermont Medical Attorney-in-Fact(s) to consult with over the medical treatment decisions that must be made on your behalf. Notice, such Parties here will not obligate the Vermont Health Care Agent (or Co-Agents) to consult these Parties.
(24) Undesired Influences. You may wish your Vermont Medical Attorney-in-Fact(s) to discount, disregard, or even avoid the influence of certain people (i.e., you are aware they are strongly against your health care preferences). Document the full name and contact information that you wish the Vermont Health Care Agents to avoid or disregard when determining your health care options and decisions.
(25) Approval For Disclosure. Your approval will be needed for your Vermont Health Care Agents to release any medical information to Adults and Minors. List each Person that is allowed to receive information about your medical condition from your Vermont Health Care Agents.
(26) Forbid Interference. You may be definitive on who may not interfere with the appointment and directives you set in this form. List each Party that should not be given a say in your treatment directives by name and address. While the room to record one Party is immediately available, you may forbid as many people as you like from interfering with this form and the decisions of your Vermont Health Care Agent(s) using an attachment.
(27) Vermont Court-Appointed Guardian. If Vermont Courts determine that a Guardian must be appointed, they can turn to this document for your nomination. You may indicate that you wish your Vermont Health Care Agent by selecting the appropriate statement.
(28) Unique Guardian Nomination. If you wish to nominate someone other than your Vermont Health Care Agent for the court to consider appointing, then choose the second directive. Additionally, make sure to dispense your Nomination’s full name, complete address, and current telephone number.
(29) Alternate Guardian Nomination. If the Courts do not intend to appoint the nomination made above as your Guardian or if your Nomination is unavailable for this role, then you may nominate an Alternate Preferred Guardian(s) by presenting each one’s name, address, and phone number in the space provided. If naming more than one, list them in the order you wish them approached.
(30) Prevent An Unwanted Court-Appointed Guardian. If the Courts decide to appoint a Guardian of your person but will not honor your nominations, you may still prevent specific Parties from being considered. Every Party that you would not want as a Vermont Court-Appointed Guardian should be presented by name with his or her address and phone number.
(31) Vermont Patient Identity.

Part 3 Statement Of Values And Goals
(32) Discussion Of Personal Values. You may wish to make sure your Vermont Health Care Agents are absolutely sure of what you consider important regarding your quality of life and your medical care. Use the area provided to present this report. This is a good idea even if your Medical Attorney-in-Fact and Co-Agents are up-to-date on your ethics and values in medical treatment and surviving severely traumatic medical events since it will provide a valuable framework in a stressful decision-making process for your Agent(s) to operate under.
(33) General Advice To Agents. A valuable tool that you can pass to your Vermont Medical Attorneys-in-Fact can take the form of some basic advice on how they should interpret your value system when it comes to your quality of life and treatment preferences. Your advice or suggestions can be useful because serious medical conditions can often be accompanied by unforeseen complications requiring the Agent(s) to make decisions that you have not necessarily discussed. For instance, you may document which of your beliefs would take precedence over the other if two or more should conflict.
(34) Identify Vermont Patient.

Part 4 End Of Life Treatment Wishes
Choose Only Item 35 Or Attend To Items 36 Though 48
(35) Prolonging Life When Close To Death. If you have a medical condition that renders you close to death or unconscious, then you have the option to pre-authorize life-sustaining procedures (i.e., machinery, medications, etc.) as well as inform Vermont Medical Staff that you wish your life sustained when your body can no longer maintain itself. Both of these goals can be accomplished by initialing the first Directive in Part 4.

(36) Denying Life-Support Procedures and Medications. Directive 2 provides the statement needed to inform Vermont Medical Providers of your decision to deny the life-sustaining treatments you would deny. Initial the first statement in Directive 2 to claim this declaration as your own.
(37) Striking Certain Life-Sustaining Procedures. Continue to initial each medical treatment that should be discontinued when you are near death or declared unable to regain consciousness. Using this list, you may choose to deny the use of breathing machines, the administration of tube feedings through a machine, antibiotics, medications carrying the goal of (only) extending your life, and “Any Other Means.”
(38) Other Denied Treatments. The list accompanying Directive 2 presents its final option as “Other.” You may use this area to document any treatment, medication, or procedure that you do not wish instituted to extend your life on the blank line provided. If you include this statement, make sure to initial the blank space preceding it to show Vermont Medical Professionals that you have approved its inclusion.
(39) Vermont Health Care Agent Decision. If you wish your Medical Attorney-in-Fact to make the decision on which treatments should be administered when you will no longer regain consciousness and/or are close to death, then you must initial Directive 3. Notice that here, your Vermont Medical Attorney-in-Fact or Health Care Agent will also have the ability to decide on whether artificial nutrition and hydration should be delivered by tube from a machine.
(40) Dignity, Comfort, And Relief. Directive 4 specifically requests that Vermont Medical Professionals maintain your appearance, comfort, hygiene, and other concerns that will maintain your dignity and comfort or pain levels.
(41) Pain Medication Directive. You may give the authorization to manage your pain and comfort with pain medication (even those with rare or unforeseen side-effects that hasten your death) by initialing Directive 5.
(42) Hospice Care. If you are close to death, then you may opt to be placed in a Hospice. Some may consider this wise since it may make the process of dying more comfortable or even less stressful. To issue this desire, initial Directive 6.
(43) End-Of-Life Residence. Initial Directive 7 if you intend to experience your end-of-life event in your home (Note, this may not be possible for some conditions).
(44) Other Wishes And Instructions. You may continue declaring your medical care needs by documenting your requests to the space available in Directive 8. Once this is done, make sure to provide your initials as confirmation to the additional provision(s).
(45) Vermont Patient Identity.

Part 5 Other Treatment Wishes
(46) Do Not Resuscitate Order. Directive 1 of Part 5 requests that you have a DNR written for you if you have not issued one already, are unconscious, and/or suffering a debilitating and untreatable medical condition. Produce your initials to make this statement.
(47) Trial Period For Critical Health Crisis. Produce your initials to Directive 2 if you wish to receive life-sustaining treatments if it is unknown whether you can recover or not.
(48) Refusing Specific Treatments When Unable To Think Or Act For Yourself. If you are conscious but incognizant or unable to live independently, then the option to refuse invasive life-sustaining treatments is available to you as a Vermont Patient. To deny a specific treatment, review the list provided then place your initials next to each life-extending treatment you do not wish to receive or wish discontinued when you are declared as unable to comprehend your surroundings or act for yourself. You may use this list to deny the use of breathing machines, feeding tubes, antibiotics, life-extending medications, any treatment that holds the goal of keeping you alive longer, and/or any treatment you define in the space labeled “Other.”
(49) Costs, Risks, And Burdens That Disqualify Life-Sustaining Treatment. Quite a few life-sustaining treatments administered to Patients with life-long severely debilitating injuries or illnesses with no cure or who have been deemed as permanently unconscious can be extremely burdensome. They may come with an unmanageable cost or significant risk to the Patient’s life and/or quality of life. Any life-extending treatments that you do not wish to undergo, regardless of your condition, because the risk or burden (i.e., on your finances, health, or quality of life) should be listed as such in the area provided.
(50) Pregnancy Directive. If there is a chance that you may be permanently incapacitated or unconscious either while or after you have become pregnant, then initial Directive 5.
(51) All Life-Sustaining Treatment When Pregnant. Initial the appropriate statement to authorize and request all life-sustaining treatments to be administered if you are permanently unconscious or incapacitated.
(52) Specific Authorized Treatments. You may request only certain life-sustaining treatments to be given when you are incapacitated or unconscious and pregnant by producing your initials of approval next to each statement in this item. Every statement that bears your initials will be considered a life-sustaining treatment that you wish to receive when necessary if you are pregnant and incapacitated without a cure or permanently unconscious. If desired, you may request specific treatments by initialing the “Option” statement, then presenting your request on the blank line provided
(53) Denying Life-Sustaining Treatment When Pregnant. A statement enabling you to deny all life-sustaining treatment when you are permanently incapacitated and/or unconscious while pregnant has been provided. Initial this item to set this directive in place.
(54) Preferred Vermont Medical Facilities. If you prefer to be treated in a specific Hospital or Medical Facility, then you may utilize Directive 6 of this area to document your preference by dispensing the name, address, and telephone number of the Hospital or Medical Care Facility you prefer to receive care from. There is enough space to name two such preferred institutions.
(55) Denying Medical Facilities. To avoid or deny receiving care from a specific Hospital or Medical Facility, continue through Directive 6 where an area has been provided to name a Medical Facility you wish to avoid and present the reason for your reluctance or denial.

(56) Preferred Medications Or Treatments. You can document the medications or treatment programs that you feel best works for your medical condition or those that you approve of and anticipate requiring should a medical event leave you in a lifelong condition where you are unable to think or act for yourself or leaves you permanently unconscious.

(57) Disapproved Medications And Treatments. Utilize the space provided in Directive 7 to provide a detail of the medical procedures and medications that you feel strongly against or are known to affect you in a negative or painful way. In addition to dispensing the name of the medication or procedure you do not authorize, give the reason why you wish Vermont Medical Professionals to avoid administering them.
(58) Student Medical Education. Indicate whether you approve of participating in Student Medical Education Programs by initialing the first statement in Directive 8 then selecting the appropriate phrase to define whether you authorize or disapprove of receiving treatment from Student Medical Education.
(59) Student Treatment Studies. If you wish to approve or deny the use of Treatment Studies and Drug Trials administered as part of your health care, then initial the second statement made and circle the phrase that best describes your intent.
(60) Vermont Health Care Agent Decision. The Vermont Health Care Agent can be authorized to decide upon whether Student Medical Education, Treatment Trials, or Drug Trials can be administered to treat you.

(61) Mental Health Treatment. You can utilize Directive 9 to address the possibility of requiring Mental Health Treatment when you are suffering an emergency and must be involuntarily treated at the time. By numbering the treatments, you approve of receiving by listing the treatment you prefer most numbered as “1,” the treatment that you prefer after your listed first choice as “2,” and so on. You may leave disapproved treatments blank if preferred but it is recommended that you assign a number to all possible procedures and treatments. In this way, you may retain control over a potentially hazardous mental health crisis by informing Vermont First Responders and Medical Personnel of the treatment measures that you prefer and those you wish to be applied as a last resort or even avoided. You may also present your own mental health treatment preference in the order you wish by placing the appropriate number next to “Other” then using the space provided to detail the desired treatment.
(62) Refusing All ECT. A standard treatment response to some mental health issues involves administering electro-shock treatment or ECT. Some Vermont Patients find this to be an invasive procedure therefore the opportunity to inform attending Vermont Health Care Professional that you do not authorize or consent to any form of ECT has been provided. Initial this statement to include it in your directives.
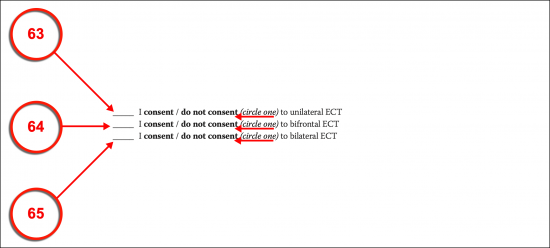
(63) Unilateral ECT. You may issue a directive on unilateral ECT sessions by initialing the appropriate statement then indicating whether you will consent to this procedure or not by selecting one of the bold phrases displayed (“Consent” or “Do Not Consent”).
(64) Bifrontal ECT. The next statement on this topic enables your decision on bifrontal ECT sessions to be presented as treatment that you will provide consent to receive or will not consent to receive.
(65) Bilateral ECT. You may consent or refuse to receive bilateral ECT treatments by initialing the statement on this subject then selecting the appropriate phrase.
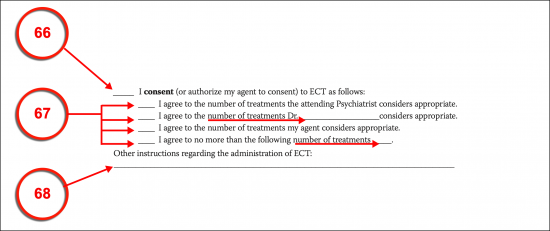
(66) Vermont Health Care Agent Power To Decide. Your Vermont Health Care Agent can be authorized to decide upon the administration of ECT as part of your mental health treatment (when necessary) by initialing your authorization for this power.
(67) Approved Number Of ECT Treatments. The number of ECT treatments that your Agent may consent to on your behalf should be discussed. Several statements for this power are provided to aid in your definition. Review these options then initial the one that is an accurate representation of your intent. In this way, you may set the authorized number of ECT treatments to be determined by the attending Psychiatrist, as directed by a specific Physician or Psychiatrist that you name, decided by your Vermont Medical Attorney-in-Fact or Health Care Agent, or you may set a predetermined number of ECT sessions to the final statement. If you decide to choose more than one of these statements as appropriate, then you must explain how these consents interact in the next area
(68) Additional ECT Instructions. If there are any concerns or directives left unaddressed concerning the administration of electroconvulsive therapy, then dispense such provisions to the area provided.
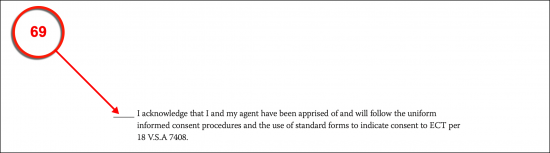
(69) Informed Consent Acknowledgment. You must provide your initials to solidify that your ECT directives have been made in compliance with 18 V.S.A 7408 (found under Title 18 Chapter 177 in the Vermont Statutes).
(70) Vermont Patient Information.

Part 6 Waiver Of Right To Request Or Object To Future Treatment
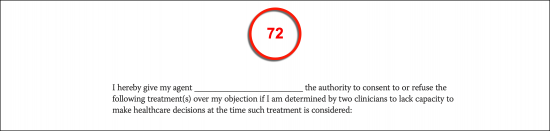
(71) Vermont Health Care Agent Name. Produce the full name of the Vermont Health Care Agent that you authorize to supersede your medical requests during a time of crisis. This can be useful during events when you are faced with a treatment that is painful during a time when you are unable to make reasonable and informed decisions. When you are in such a state, then some of your decisions may be counter-productive to your chances of survival or your preferences when cognizant and reasonable.

(72) Confirm The Overriding Agent’s Name. To confirm your Agent’s right to override your medical instructions during a time of crisis (i.e., a traumatic mental health crisis) record his or her name to the declaration statement provided.
(73) Solidify The Power Of This Declaration. If you have named a treatment in this directive that you wish to receive even over your refusal at the time of its administration but are absolutely sure it must be received for your survival, then you must confirm such authorization here and now. To do so, list each treatment that must be administered under any circumstances when needed.
(74) Unequivocally Deny Treatments/Medication. Similarly, you may override your own requests for inappropriate treatment (when under duress) by denying its application here. To this end, list every medical procedure or medication that you do not authorize regardless of the situation.
(75) Agent Power Of Medical Facility Admission. You may either allow your Vermont Health Care Agent to override your preferences on where you may receive your health care or treatment, or you may insist that the directives you have set remain in place regardless of your medical condition. To give your Vermont Health Care Agent this authority select the “Yes” line, otherwise, select “No” to limit his or her decision-making powers in this matter.
(76) Agent Power For Voluntary Discharge Of Mental Health Care Facility. This document will enable your Vermont Health Care Agent to override your decision to discharge yourself from a Mental Health Facility or program that you have volunteered to enter by selecting the “Yes” line. If your Vermont Health Care Agent should not have this ability, then initial the “No” line.
(77) Confirming Signature For Part 6. Since Part 6 will determine if or when your directives can be overridden by your Vermont Health Care Agent, your authorizing signature will be needed along with your signature date.
Acknowledgments
(78) Vermont Attorney-in-Fact Acknowledgment. Each Health Care Agent should formally accept the responsibilities that accompany this role. He or she will be wielding your authority to make health care decisions when you are unable to. Thus, your Vermont Health Care Agent (and Co-Agent) should read this document carefully, then sign his or her name.
(79) Vermont Attorney-in-Fact Information. Each Signature Vermont Health Care Agent must provide his or her printed name, address, and telephone number after signing his or her name.
(80) Alternate Vermont Agent Acknowledgement. Since your Vermont Alternate Agent may be needed to step into the Medical Attorney-in-Fact or Health Care Agent role, each Alternate Agent you have named must sign his or her name.
(81) Alternate Vermont Agent Information. Once he or she signs the acknowledgment, the Signature Alternate Vermont Agent(s) must dispense the address and phone number that should be used to initiate contact regarding this appointment.
(82) Physician Acknowledgement. Every Primary or Preferred Physician named in this document should sign it, document his or her formal title, submit the Facility address and phone number where he or she can be reached, and record the signature date.
(83) Facilitator Acknowledgement. If a Third Party was needed to explain Part 6 of this document, then his or her signature, formal job title or professional position, and signature date must be included with these acknowledgments.
(84) Patient Identity.

Part 7 Organ And Tissue Donation
(85) Vermont Organ Donation Declaration. To become a Vermont Organ Donor, initial the declaration on display then continue to select the level of anatomical gifts you wish made. You may choose to donate all your organs and tissues, only major or vital organs, only tissues (i.e., bone or skin), eye tissues, let your Vermont Health Care Agent decide on your organ donation, or you can provide your own directions on which anatomical gifts can be made by selecting the final option and using the space provided for this report.
(86) Donation For Science. You can declare that you also wish to donate your body to science (i.e., education) by initialing this directive.
(87) Opting Out Of Anatomical Gifts. If you do not wish to make any anatomical gifts or organ donations, produce your initials to the final directive on this page. If this is the case, do not initial the above organ donation statements.
(88) Vermont Patient Name

Part 8 Disposition Of Body After Death
(89) Disposition Of Remains After Death. Three options are available to dictate how you wish your remains handled. You can request a funeral by initialing the first statement then dispensing the name of the burial plot you have purchased (if relevant).
(90) Specific Directions On Cremation. If you have determined that you wish to be cremated then, by selecting the second statement of this directive you may request that you be cremated and where you wish your ashes to be buried/dispersed.
(91) Agent Or Family Decision Power. The third option allows you to declare that you wish your Vermont Health Care Agent or a Family Member to handle the disposition of your body according to the instructions you provide directly to the space available.
(92) Vermont Medical Attorney-in-Fact Power. If you wish your Vermont Health Care Agent to handle your post-death arrangements, then initial the statement displayed in Directive 2 of this section.
(93) Separate Appointment. If you have determined that a Party that you name should be in charge of your remains after death, then initial the second statement of the second directive. This also requires that you document his or her full name, address, and phone number.
(94) Designating Your Family. If you wish your Family to decide on your disposition, then initial the final statement of Directive 2
(95) Autopsy Directive. Indicate if you would approve of an autopsy or prefer your Vermont Health Care Agent to decide on this issue by initialing your approval to the appropriate statement in Directive 3.
(96) Preset Arrangements. If you have already completed arrangements for your remains with a funeral/cremation service then furnish the name, address, and telephone number of the Post-Death Entity these arrangements were made with. Use the space in Directive 4 for this purpose.
(97) Vermont Patient Information

Part 9 Signed Declaration Of Wishes
(98) Vermont Principal Signature Execution. Sign your name and deliver the current date to this document while two Witnesses attend and observe your signature’s execution.
(99) Agent Distribution Acknowledgement. If you have given (or intend to give) your Vermont Health Care Agents, Co-Agents, and Alternate Agents a copy of this document then, it is recommended you declare this distribution occurred by signing and dating the declaration made.
(100) Doctor Or Clinician Distribution Acknowledgment. Sign and date the optional declaration statement if you wish to verify that you will give (or have given) your Doctor/Clinician a copy of this form.
Acknowledgment Of Witnesses
(101) Witness One Acknowledgement. The first Witness to take this document (after watching you sign it) should produce his or her signature, printed name, and signature date as proof that the affirmation statement made is accurate.
(102) Witness Two Acknowledgment. The second Witness to gain control of this document must also provide his or her signed and printed name then present the current date to show his or her agreement to the affirmation made regarding your signature.
(103) Facilitator Acknowledgment. If a Facilitator employed by a Hospital or Health Care Facility where you are being treated aided you in executing this document (i.e., they have explained it to you, aided you in its preparation, etc.), then he or she must acknowledge this role by submitting his or her signed name, title, address, contact number, and signature date.
(104) Distribution List. Initial each location or Recipient who will or has received a copy of this directive. If relevant, make sure to dispense the name and address of each Family, Member, Physician (“MD”), Hospital, and any other Party that will possess a copy of this document.
Related Forms
 Durable Financial Power of Attorney
Durable Financial Power of Attorney
Download: PDF, MS Word, OpenDocument

Download: PDF, MS Word, OpenDocument