Updated August 09, 2023
A South Dakota medical power of attorney lets a principal select an agent to handle medical-related decisions on their behalf. The principal can also give end-of-life treatment options to be at the sole responsibility of the agent. The principal can also list special requests and their preferences for treatment. Successor agents may also be included if the primary agent is not available.
Laws
- Signing Requirements – Two (2) witnesses or a notary public (§ 59-7-2.1).
- Statutes – Chapter 59-7 (Termination of Agency)
How to Write
Download: PDF, MS Word, OpenDocument
1 – Download The Paperwork To Appoint A Health Care Attorney-in-Fact
Download the document available through one of three buttons furnished with the image below. If you intend to prepare it onscreen make sure you have a program compatible with the version, you have selected.
2 – A Formal Declaration Statement Will Require The Party Identities Supplied
The first set of blank lines in this document will need to establish who the Principal is, who the Health Care Attorney-in-Fact is, and who the Successor Agent(s) is. Find the first empty line under the title “Durable Power Of Attorney For Health Care” then produce the Principal’s Legal Name. This individual is the person who intends to allow another entity to make Health Care Decisions on his or her behalf when incapacitated. 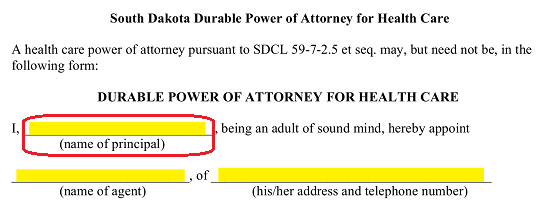 The Full Name of the Health Care Attorney-in-Fact should be placed on the empty line between the words “…Hereby Appoint” and “Of.” The Health Care Attorney-in-Fact will be the person who will have the Principal Power to make Health Care Decisions on behalf of the Principal should the Principal be unable to communicate due to a Medical Event.
The Full Name of the Health Care Attorney-in-Fact should be placed on the empty line between the words “…Hereby Appoint” and “Of.” The Health Care Attorney-in-Fact will be the person who will have the Principal Power to make Health Care Decisions on behalf of the Principal should the Principal be unable to communicate due to a Medical Event.  Use the empty line labeled “(His/Her Address And Telephone Numbers)” to document the Health Care Attorney-in-Fact’s Residential Address and Current Telephone Number. It is important this Contact Information is up-to-date and accurate.
Use the empty line labeled “(His/Her Address And Telephone Numbers)” to document the Health Care Attorney-in-Fact’s Residential Address and Current Telephone Number. It is important this Contact Information is up-to-date and accurate.  If the Principal wishes to have a Successor Agent in place, this must also be declared. There will be a specific area where this entity can be named. Locate the blank line labeled “Name Of Successor Agent” then enter the Name of the individual who may assume Principal Health Care Powers should the Health Care Attorney-in-Fact be unwilling or unable to act as the Principal’s Health Care Attorney-in-Fact. This entity’s Address and Telephone Number will need to be entered on the next empty line.
If the Principal wishes to have a Successor Agent in place, this must also be declared. There will be a specific area where this entity can be named. Locate the blank line labeled “Name Of Successor Agent” then enter the Name of the individual who may assume Principal Health Care Powers should the Health Care Attorney-in-Fact be unwilling or unable to act as the Principal’s Health Care Attorney-in-Fact. This entity’s Address and Telephone Number will need to be entered on the next empty line.
3 – Supply Any Limitations Or Additional Directives The Principal Wishes Applied
The language in this document will assign the Health Care Attorney-in-Fact the Power to make Health Care Decisions for the Principal including those requiring the withholding of treatment or artificial nutrition/hydration depending on the circumstances. The default language assigning such Power is presented immediately after the identification of each party. The Principal should set aside some time to review the information here. The Principal can adjust the Powers given to the Health Care Attorney-in-Fact by initialing the statements at its conclusion.
If the Principal grants the Health Care Attorney-in-Fact with the Principal Power to withhold Artificial Nutrition/Hydration when the Health Care Attorney-in-Fact believes it is appropriate to do so, the Principal should initial the first statement. The Principal can refrain from delivering the Authority the Health Care Attorney-in-Fact requires to withhold Artificial Nutrition/Hydration by initialing the second statement.
The Principal can refrain from delivering the Authority the Health Care Attorney-in-Fact requires to withhold Artificial Nutrition/Hydration by initialing the second statement.  If the Principal has determined additional Decisions the Health Care Attorney-in-Fact may make on his or her behalf should be within this Agent’s Power, these additional Powers should be reported on the blank line after the words “I Authorize The Following” and the Principal’s initials should be supplied on the empty space just before this statement.
If the Principal has determined additional Decisions the Health Care Attorney-in-Fact may make on his or her behalf should be within this Agent’s Power, these additional Powers should be reported on the blank line after the words “I Authorize The Following” and the Principal’s initials should be supplied on the empty space just before this statement.
In addition to these statements, the Principal can deliver additional instructions that he or she expects followed to the Health Care Attorney-in-Fact. Such instructions should be supplied to the blank lines under the sentence beginning with the words “I Give The Following Instructions….”
4 – The Principal Must Supply This Document With A Verifiable Signature
The Principal must Date and Sign this template once it has been completed to his or her satisfaction. This Signature must be either Witnessed by two people or performed in the presence of a Notary Public. Locate the Signature Area near the bottom of this page.
The first item the Principal should be attended to is the “Date” line. The Principal must enter the Calendar Date he or she signs this document on this line.
 The Principal will be required to sign the blank line labeled “Your Signature”
The Principal will be required to sign the blank line labeled “Your Signature” After presenting the Signature Date and his or her Signature, the Principal must print his or her Address and Full Name on the blank lines labeled “Your Address” and “(Type Or Print Your Name), Principal.”
After presenting the Signature Date and his or her Signature, the Principal must print his or her Address and Full Name on the blank lines labeled “Your Address” and “(Type Or Print Your Name), Principal.”  As mentioned earlier, one of two options is available for authenticating this Signature. Each option will have an area designated purely for this purpose. The first option will be that of Notarization. If a Notary Public has been obtained for the signing, the Principal should release this document to him or her after signing it so that it may be notarized.
As mentioned earlier, one of two options is available for authenticating this Signature. Each option will have an area designated purely for this purpose. The first option will be that of Notarization. If a Notary Public has been obtained for the signing, the Principal should release this document to him or her after signing it so that it may be notarized.  If the Principal has elected to sign this paperwork before two Witnesses, the Principal should sign turn this document over to the Witnesses so they may attend to the section below the heading “Statements Of Two Witnesses” then each Witness must Sign his or her Name, then Print his or her Address and Name. Each Witness will have his or her own area to attend to below the statement “The Principal Voluntarily Signed This Document In My Presence”
If the Principal has elected to sign this paperwork before two Witnesses, the Principal should sign turn this document over to the Witnesses so they may attend to the section below the heading “Statements Of Two Witnesses” then each Witness must Sign his or her Name, then Print his or her Address and Name. Each Witness will have his or her own area to attend to below the statement “The Principal Voluntarily Signed This Document In My Presence”