Updated October 22, 2023
A North Dakota advance directive is a document that allows a person to appoint a health care agent to take care of their medical needs and make their end-of-life treatment plans. An advance directive lets a person make their medical goals known to family members and medical staff. The agent selected is expected to align their decision-making process with the goals of the person who wrote them.
Four (4) Parts
- Health Care Directive (‘power of attorney’);
- Health Care Instructions (‘living will’);
- Making an Anatomical Gift; and
- Making the Document Legal.
Laws
Statute – § 23-06.5-01 to § 23-06.5-19 (Health Care Directives)
Signing Requirements (§ 23-06.5-05) – Two (2) witnesses or a notary public.
State Definition – (§ 23-06.5-02(5)) – “Health care directive” means a written instrument that complies with this chapter and includes one or more health care instructions, a power of attorney for health care, or both.
Versions (5)

Download: PDF

Download: PDF

Download: PDF
Download: PDF

Download: PDF
Table of Contents |
How to Write
Download: PDF, MS Word, OpenDocument
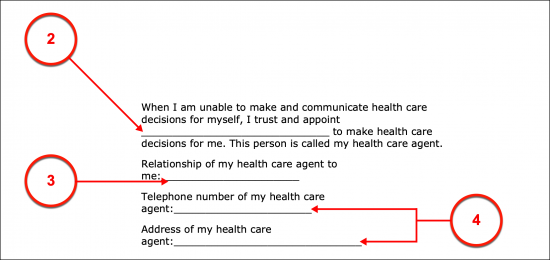
(1) North Dakota Principal. As the potential (or current) Patient appointing a Health Care Agent in the State of North Dakota, document your full name. This will allow you to assume the role of the North Dakota Declarant or Principal who is establishing his or her health care preferences through this document.
(2) North Dakota Health Care Agent. The North Dakota Health Care Agent can only act as your Health Care Agent in this state, if he or she is deliberately assigned this role. Therefore, deliver his or her full name to the statement of appointment being made.
(3) Health Care Agent Relationship. The North Dakota Health Care Agent’s relationship to you, the Principal or Declarant, should be presented as part of this appointment process.
(4) North Dakota Health Care Agent Contact Information. The North Dakota Health Care Agent’s permanent address and contact telephone number(s) are required for this paperwork. This will aid in identifying and contacting this Party when needed.
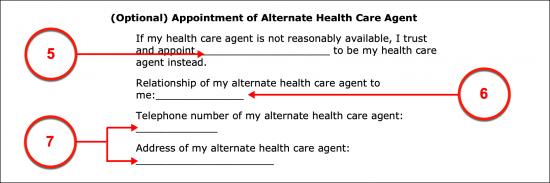
Appointment Of Alternate Health Care Agent
(5) Alternate North Dakota Health Care Agent. You can name an additional Party to the North Dakota Health Care Agent position that will only be held in reserve in case the currently appointed North Dakota Health Care Agent above is unable or unavailable to represent you when you are unconscious and requiring someone to dispense your treatment preferences to North Dakota Physicians. The Party you name as your North Dakota Alternate Agent can readily assume the powers delivered through this document and step in on your behalf but only if he or she is formally appointed with this ability by a presentation of his or her full name.
(6) Relationship To Principal. The way in which the North Dakota Alternate Agent is related to you (the Principal) should be established. For instance, he or she may a spouse, a sibling, a parent, a trusted friend, etc.
(7) Contact Information Of North Dakota Health Care Agent. Furnish the North Dakota Alternate Health Care Agent’s address and telephone number so that he or she can be contacted using this document.
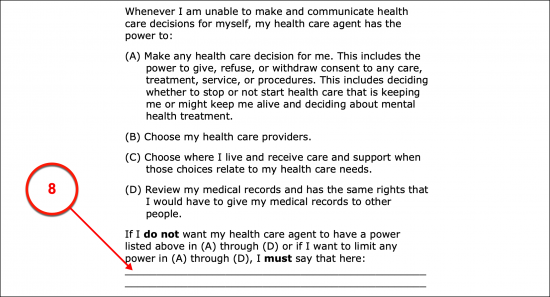
Limits To Default Health Care Agent Powers
(8) Principal Limitations On Health Care Agent. While the default principal powers this document assigns to the North Dakota Health Care Agent are fairly basic, they are sweeping. This document enables you to control your Agent or limit these powers in a space reserved exclusively for this purpose. Review the list of these powers (lettered A through D) then either strike out the ones that should not be granted or produce a report on how you would like the North Dakota Agent to handle these powers. If desired, you can simply state that you do not grant your Health Care Agent the powers in a specific item or document how you would like the powers available to be limited or restricted from his or her use. If more room is needed in the space provided, then attach a document where you have presented the remainder of your limitations or instructions to the North Dakota Health Care Agent.
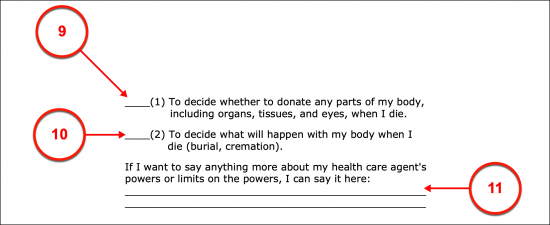
Health Care Agent’s Post-Death Power
(9) Organ Donation. The ability to represent you after death is not a default power granted to the North Dakota Health Care Agent. Actions such as donating your organs or making anatomical gifts on your behalf after death must be approved by you (as the North Dakota Principal). Statement 1 provides the needed language to grant the North Dakota Health Care Agent the power to decide on your organ donations but requires your initials of approval to be included in this document. To prevent your Agent from making this type of decision, do not initial this statement.
(10) Disposition. Outside of anatomical gifts, the Party who controls what happens to your body after death (i.e., burial, green burial, cremation, etc.) can be your North Dakota Health Care Agent provided you initial Statement 2 to give him or her the required authority to decide and act upon your body’s disposition on your behalf after death.
(11) Post-Death Preferences Of Principal. Any additional powers, requests, or instructions that should be delivered to your North Dakota Health Care Agent should be dispensed to the area provided.
Part II Health Care Instructions
(12) Principal Goals. Any goals that you wish North Dakota Physicians to assign to treatment plans being developed when you are incapacitated, unconscious, at an end-of-life, event or any other significant event can be documented as a message or instructions to your Health Care Agent. It is strongly recommended that you complete this and the following areas in Part II as they will aid your North Dakota Health Care Agent in determining the next course of action in a situation where you are uncommunicative as well as solidify your preferences to Reviewers of this document.
(13) Principal Concerns. Natually, experiencing the end-stages of an end-of-life event or a neurodegenerative disorder can be a very worrisome scenario. If you wish your North Dakota Health Care Agent to be aware of your fears or concerns when his or her representation is required, then present them for his or her review and use.
(14) Spiritual Or Religious Beliefs. Any concerns regarding your religious or spiritual beliefs that you wish observed or taken into strong consideration when unable to communicate and enduring a medical event can be established for your North Dakota Health Care Agent’s review in the second topic of discussion presented in Part II.
(15) Quality Of Life Statement. Your quality of life may be a significant concern. If you have health care preferences or definitive statements that define when you believe life should not be prolonged, then document such directions. For instance, if the price of recovering from a terminal disease will prove over burdensome, carry a slim to no chance of success, cause permanent intolerable pain, and/or leave you unable to survive, then you may wish such treatment denied. In such a scenario, discuss the medical condition of concern then the treatment and recovery circumstances that you will not tolerate or want to be authorized by your North Dakota Health Care Agent.
(16) Directives For Family. If you wish your North Dakota Health Care Agent to interact with your family members or if you anticipate your family members contacting him or her when you are incapacitated, then you can include a discussion on how you wish your North Dakota Health Care Agent to interact with them. For instance, you may wish him or her to consult a Family Member before making treatment decisions.
(17) Chances For Recovery. As mentioned before, your North Dakota Health Care Agent may need to make decisions concerning your period of recovery (or post-recovery) for you when you are completely unable to communicate with him or her (or anyone else). Thus, a space has been included so that any directions or messages you wish the North Dakota Health Care Agent to operate with can be documented.
(18) Directives When Terminal. Your North Dakota Health Care Agent should be kept informed of your preferences when you have been diagnosed with a fatal medical condition that results in death. If this happens and you lose consciousness or are unable to communicate for a significant period of time (or permanently), then it will be up to your Health Care Agent to inform North Dakota Physicians of your treatment preferences when you are in such a scenario. By documenting such preferences, a clearer understanding of your wants, needs, authorizations, and preferences can be set to paper to promote your North Dakota Health Care Agent’s ability to represent them
(19) Instructions For Permanent Unconsciousness. Present any general or specific instructions that you expect observed when you are permanently unconscious.
(20) Dependency. Inform your North Dakota Health Care Agent (and other Reviewers of this paperwork) of the decisions or medical preferences you have if you are rendered completely dependent on others and unable to represent yourself as a result of being incognizant, unaware, or unconscious.
(21) Pain Management. Some medical conditions may result in an intolerable amount of pain to your body even when you are unconscious (as well as unaware of your surroundings or incognizant). Since there is a wide range of pain management medications and techniques, it is strongly recommended that you document any preferences, instructions, limitations, or restrictions that you want applied to pain management courses that may be used.
(22) Physician Preference. If you have a Primary Physician that you wish to be treated by when incapacitated, then present his or her full Name, the Office or Institution where he or she practices, as well as the address and phone number needed to contact him or her. This may be particularly useful if you are incapacitated and hospitalized while unaware, unconscious, or unable to communicate.
(23) Facility Preferences. Document the name of the Health Care Facility (i.e., a Hospital) where you prefer to receive treatment. Make sure to include its address and phone number(s).
(24) Hospice Instructions. You can use this paperwork to also instruct your North Dakota Health Care Agent on where you wish your end-of-life event (dying) to occur. If you are unable to voice or communicate our wishes when death is near, this area will inform your North Dakota Health Care Agent how to proceed as well as confirm your wishes to Reviewers.
(25) Discussing Post-Death. If you have given the North Dakota Health Care Agent the authority to handle your body after death, then use the space provided to provide details as to how you wish your remains to be handled and put to rest.
(26) Additional Declarations. The topics set here allow a comprehensive set of instructions and directives to be established, however, if you have any additional treatment, recovery, or disposition concerns that have not been documented, then use the space provided.
Part III. Making An Anatomical Gift
(27) Anatomical Gift Discussion. You can volunteer to donate your organs and other tissues or body parts through this directive. To do so, initial either the first statement in Part III to make any and all anatomical gifts needed at the time of death or initial the second statement in this section to specify that only certain organs and/or tissues are authorized for donation.
Part IV Making The Document Legal
(28) Signature Date. Your signing of this form will represent your authorization of its contents as being accurate. It is generally important to Reviewers that such an act is easily verified. This requires that your signature be verified by two Witnesses or a Notary Public as being provided on a specific calendar date. Report this date.
(29) Principal Residential Information. Document the city and state of your residence.
(30) North Dakota Principal Signature. Your signature is required for this document to become an active directive. If you have opted to have your signature notarized, then follow the directions of your Notary Public. If you have opted to have your signature Witnessed then, surrender this document to Witness 1.
Option 1 Notary Public
(31) Notarization. The North Dakota Notary Public will use his or her appointment to notarize your signature. This will provide proof that you willingly signed this form with a complete understanding of your actions. Be advised, you may not obtain a Notary Public that is related to you. Instead, a completely impartial Party must be obtained.
Option 2: Two Witnesses
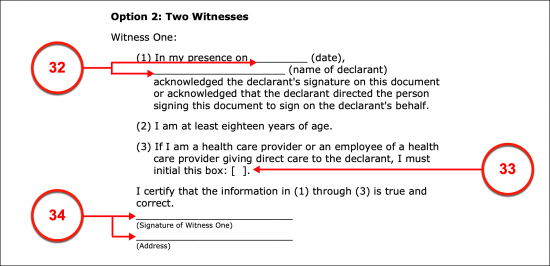
(32) Report Of Principal Signing. Witness 1 should review and complete the statement devoted to his or her signature. This requires the date when you signed this form as well as your full name produced.
(33) Witness Status. If Witness 1 is employed by your Health Care Provider or is an independent Provider formally administering your care, then he or she must initial the Statement 3.
(34) Witness 1 Signature. Witness 1 must sign his or her name then present the address where he or she can be reliably contacted.
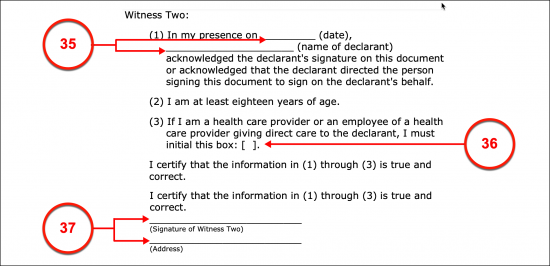
(35) Record Of Principal Signing. Witness 2 must also complete some items in the declaration provided for him or her to complete. Statement 1 must be provided with the date of your signing and your full name as the North Dakota Principal.
(36) Witness Status. A Health Care Provider or an Employee of the Health Care Provider responsible for your care can act as a witness to your signature but must self-identify as carrying this status. This can be done with his or her initials to Statement 3.
(37) Witness 2 Signature. Witness 2 must sign his or her name to the completed statement upon review and agreement. Additionally, Witness 2 must report his or her address.
Acceptance Of Appointment Of Power Of Attorney
(38) Signature Of North Dakota Health Care Agent. The North Dakota Health Care Agent you have appointed above should read the acceptance statement the formally acknowledge it by signing his or her name.
(39) Signature Of North Dakota Alternate Agent. Once the North Dakota Health Care Agent has attended to the acceptance statement, the Alternate Agent you named should acknowledge the provided statement then agree to it by signing his or her name.
Related Forms
 Durable Financial Power of Attorney
Durable Financial Power of Attorney
Download: PDF, MS Word, OpenDocument

Download: PDF, MS Word, OpenDocument