Updated October 22, 2023
A Mississippi advance care directive is a document that allows a person to select an agent to speak on their behalf in healthcare-related matters. An advance directive is common for older people and those with high-risk health conditions. It’s a plan to prepare a patient in the event they are unconscious and unable to speak for themselves.
Advance Directive Includes
- Part 1. Durable Power of Attorney for Healthcare
- Part 2. Living Will
Laws
Statute – Title 41, Chapter 41 (Mississippi Health Care Decisions Act)
Signing Requirements (§ 41-41-209) – Two (2) qualified adult witnesses or a notary public in the state.
State Definition – (§ 41-41-203(b)) – “Advance health-care directive” means an individual instruction or a power of attorney for health care.
Versions (5)
- AARP
- Forest Health
- Mississippi Hospice and Palliative Care
- North Mississippi Health Services
- NRC-PAD

Download: PDF

Download: PDF
 Mississippi Hospice and Palliative Care
Mississippi Hospice and Palliative Care
Download: PDF
 North Mississippi Health Services
North Mississippi Health Services
Download: PDF

Download: PDF, MS Word, OpenDocument
Table of Contents |
How to Write
Download: PDF, MS Word, OpenDocument
Part I. Power Of Attorney For Health Care
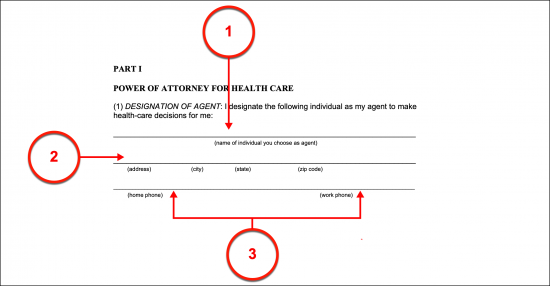
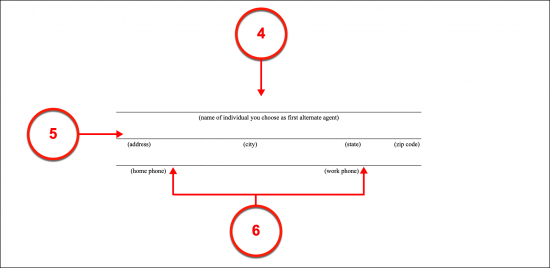
Article 1. Designation Of Agent
(1) Name Of Mississippi Health Care Agent. A Private Party of your choosing can be granted the decision-making powers you have over your health care and medical treatment so that he or she can inform Mississippi Doctors of which treatment options you would consent to. The level of this decision-making power is at your discretion, however, make sure that the Party you choose for this role is a reliable and trustworthy Entity. Document the full name of the Party you wish to act as your Mississippi Health Care Agent.
(2) Agent Address.
(3) Agent Telephone Number. In addition to the home or mailing address where your Mississippi Health Care Agent can be reached, his or her telephone number should be provided so that Mississippi Physicians can reliably initiate contact when necessary using this document. Space has been set aside for the Mississippi Health Care Agent’s home and work numbers, however, if he or she has additional contact methods (i.e., cell phone number) make sure to include this as well.
(4) Designation Of Alternate Mississippi Health Care Agent. A scenario where your Mississippi Health Care Agent is not available to act in your name, is unwilling to deliver your medical decisions, or has even been revoked may occur. You can use the optional designation area to document the full name of someone who can step into the Mississippi Health Care Agent role should it be necessary. The Alternate Mississippi Agent is your Reserve Agent and will not be granted any power to represent you unless, you name him or her, the original choice for Health Care Agent is ineffective, and you are unable to communicate your wishes when requiring medical care.
(5) Address Of Alternate Mississippi Health Care Agent.
(6) Agent Telephone Number(s).
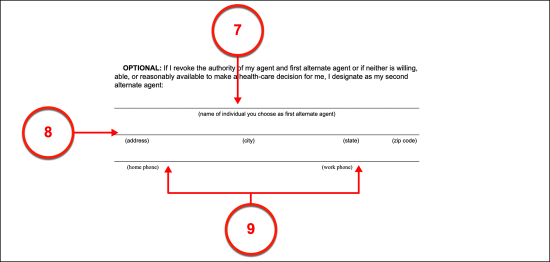
(7) Second Alternate Agent. There is always the possibility that neither your Mississippi Health Care Agent nor your First Alternate Agent are ineligible, unable, unwilling, or unprepared to wield the principal power this document grants to represent your medical directives. While this may seem improbable, to handle this possibility ahead of time, you can designate a Second Alternate Agent to step in as your Health Care Agent or Representative if needed.
(8) Second Alternate Agent Address.
(9) Second Alternate Agent Phone Number.
Article 2. Agent’s Authority
(10) Mississippi Principal Instructions. It is important that your Mississippi Health Care Agent, as well as the attending Medical Staff, have a clear idea of what you authorize your Agent to decide upon. This paperwork grants the maximum level of authority allowed in the State of Mississippi however, you can limit this or even restrict certain decisions from the Agent’s scope of principal powers by simply setting such instructions to paper. Utilize the space set aside to discuss the Agent’s principal power to decide for you and your own decisions regarding treatments you find concerning. If more room is required, you are encouraged to continue on a document that you attach to this one before it is signed.

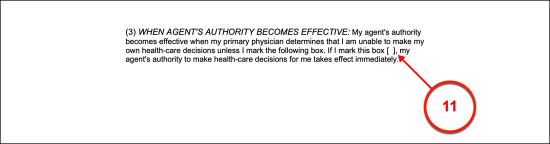
Article 3. When Agent’s Authority Becomes Effective
(11) First Day Of Agent’s Principal Powers. This paperwork will declare that the principal powers granted to your Mississippi Health Care Agent can only be accessed when your Primary Physician formally (in writing) declares that you are unable to make or convey your own medical treatment wishes. However, if preferred, you can name a specific date for these powers to go in effect in the previous section or you can mark the box in the third article’s statement to grant the Mississippi Health Care Agent the right to represent you immediately upon the execution of this document (as of the signature date of the Principal issuing it).
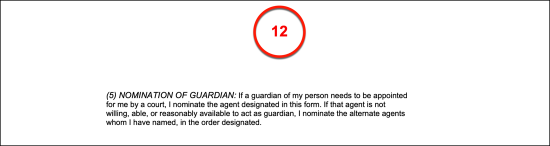
Article 5. Nomination Of Guardian
(12) Mississippi Agent As Nominee. The Mississippi Health Care Agent will be automatically nominated for the position of Court-Appointed Guardian if the court system decides it necessary. This nomination will be taken into heavy consideration in most cases but be advised, that only a court of law can decide who should be appointed as a Guardian of your person or estate. If you do not wish to nominate your Health Care Agent for the position of Mississippi Court-Appointed Guardian, then strike out the fifth article.
Part 2 Instructions For Health Care
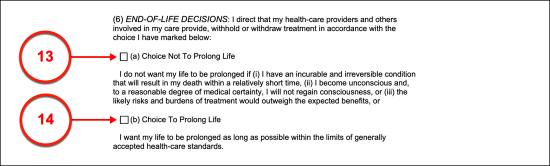
Article 6. End Of Life Decisions
Declare Item 13 Or Item 14
(13) Choice Not To Prolong Life. This section enables you to inform Mississippi Doctors of your decisions to accept life-prolonging treatments such as breathing machines, dialysis, and other life support equipment. If you wish to consent to all such treatment to maintain and extend the dying process when you are unable to communicate and have an untreatable condition (that results in death) then select the checkbox coinciding with Statement A.
(14) Choice To Prolong Life. When in a condition where there is little to no hope of recovery and death is imminent or expected shortly and you are unable to communicate then you may opt to not prolong life or extend the dying process by declaring all life-prolonging measures, techniques, and equipment be removed or denied upon such a diagnosis. By selecting Statement B, you will declare your intention to not prolong your life to the Mississippi Doctors treating you. This choice will also apply should you be rendered in a permanently unconscious (coma) state.
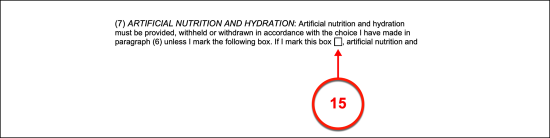
Article 7. Artificial Nutrition And Hydration
(15) Deliver Or Withdraw Consent. Mississippi Doctors will seek your stance on the delivery of food and water artificially. While assisted hand-feedings will usually be attempted if possible, some medical conditions will be accompanied by the hazard of choking when intaking food or liquid. If you wish to approve or consent to receiving your water, fluids, and nourishment artificially when needed, then place a mark in the checkbox found in the seventh article. If you do not wish to consent to the artificial delivery of fluids, water, and nutrition then leave this checkbox empty.
Article 8. Relief From Pain
(16) Pain Management In Mississippi. The option to limit or restrict pain management techniques or medications has been provided in this paperwork. This section is also useful to inform Mississippi Physicians of medications that are known to have an adverse or negative effect on your health.

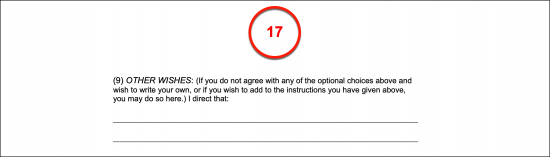
Article 9. Other Wishes
(17) Additional Mississippi Health Care Directives. You can set any legal instruction or declaration regarding your medical care, the facility that you wish to receive treatment in, your Mississippi Health Care Agent’s behavior, or even consultations that you wish your Mississippi Health Care Agent to engage in on your behalf. Document all such remaining information in the ninth article.
Part 3 Primary Physician
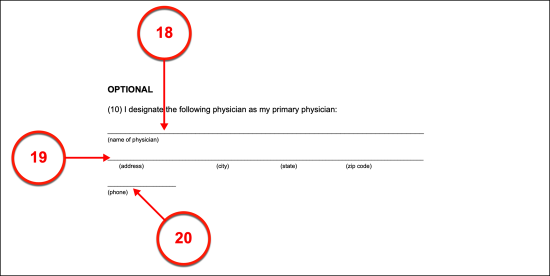
Article 10. Optional Physician Request
(18) Primary Physician Name. If you are incapacitated and wish to inform attending Mississippi Physicians that you wish to be placed under the care of your Primary Physician (or have this Party consulted if this is not possible) then, present his or her full name to this paperwork.
(19) Primary Physician Address. The address (i.e., Private Practice, Medical Center, Hospital) where your Primary Physician may be contacted should be documented.
(20) Office Or Emergency Phone Number. Produce the telephone number where your Primary Physician can be reached in a situation where you are incapacitated and require medical treatment.
(21) Alternate Primary Physician. If you would like attending Mississippi Physicians to contact another Doctor should your Primary Physician be unreachable, then use the additional space to name him or her and deliver the address of his or her Practice or Facility along with a reliable contact phone number.
Mississippi Principal Signature
Article 12. Signatures
(22) Signature Date. The current calendar date must serve as your signature date.
(23) Sign Your Name. Produce your signature to formally declare the above document as a clear representation of your medical directives. Perform this task before two Witnesses or one accredited Notary Public.
(24) Print Your Name.
(25) Complete Address. Furnish your full address and telephone number where requested.
Alternative No. 1 Witnesses
Article 13. Witnesses
(26) Date. Witness 1 of this document must record the date of his or her signature. This must be the same date as your signature date.
(27) Signature Of Witness 1. The Witnesses signing this form must attest to both your clear state of mind at the time of signing and their qualifications to fill the role of Mississippi Witness. If both these statements can be truthfully made by the First Witness, then he or she should sign this section.
(28) Printed Name Of Witness 1.
(29) Address Of Witness 1.
(30) Signature Date Of Witness 2. The next Witness must locate the area reserved for him or her then record the current date.
(31) Witness 2 Signature. Once the current date is documented, Witness 2 must sign his or her name then, continue with his or her mailing information.
(32) Printed Name Of Witness 2.
(33) Full Mailing Address.
Alternative 2. Notary Public
(34) Notary Public. If a Notary Public will be used, then this document should be given to him or her upon its execution so that the attending Notary can verify the executing signature as authentically provided by you while of sound mind.
Related Forms
 Durable (Financial) Power of Attorney
Durable (Financial) Power of Attorney
Download: PDF, MS Word, OpenDocument

Download: PDF, MS Word, OpenDocument