
Updated August 08, 2023
An Iowa medical power of attorney is a legal instrument used to defer medical decisions to a trusted person should you be incapable of communicating for yourself. This type of appointment grants power to a person you choose to make health care decisions on your behalf consistent with your wishes. It goes into effect when your attending physician determines that you can not make decisions or act on your own behalf. If you wish you may specific about your preferences in the space provided or as an attached sheet for your agent’s information.
Laws
- Signing Requirements – Two (2) witnesses or a notary public (§ 144B.3).
- Statutes – Chapter 144B (Durable Power of Attorney for Health Care)
How to Write
Download: PDF
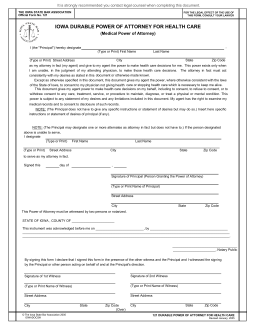
1 – The Form To Designate A Health Care Representative Is Available On This Page
You may obtain a workable copy of this form by selecting the PDF button underneath the preview image. This is located on the right-hand side of this page.
2 – Declare The Identity Of The Health Care Agent
In order for this paperwork to apply, there must be no question as to the identity of the Health Care Agent the Principal intends on assigning Principal Authority to. This issue will be nicely solved by providing the Health Care Agent’s information immediately. Locate the first blank line in the opening statement, just after the words “I (the “Principal”) hereby designate,” then fill in the First Name and Last Name of the Health Care Representative chosen by the Principal.  The next blank line calls for the Street Address, City, State, and Zip Code of the Health Care Representative to be reported.
The next blank line calls for the Street Address, City, State, and Zip Code of the Health Care Representative to be reported. 3 – Review The Principal Powers That Will Be Delivered To The Health Care Agent Through This Document
3 – Review The Principal Powers That Will Be Delivered To The Health Care Agent Through This Document
The next several paragraphs will provide a brief description of the default powers granted by this paperwork to the Health Care Agent. The Principal may believe that more definition, instruction, or limitations should be placed on this entity when wielding Principal Authority. If so, he or she may provide such preferences by reporting them in the space below the statement labeled “NOTE: (The Principal does not have to give any specific instructions or statement of desires but may do so). Insert here specific instructions or statement of desires of principal (if any).” If there is not enough room a separate sheet(s) containing the Principal’s Preferences may be cited in this space and the report attached to this form.![]() 4 – The Principal May Choose Alternate Health Care Agents As A Precaution
4 – The Principal May Choose Alternate Health Care Agents As A Precaution
This form will provide the option of naming an Alternate Health Care Agent or Attorney-in-Fact. Such an entity is expected to take on the role of the Primary Health Care Agent when or if the Primary Health Care Agent cannot fulfill it. To name an individual as an Alternate Health Care Agent, the Legal Name of the Alternate Health Care Agent by entering his or her First and Last Name on the first blank space in the second “Note.” This should be followed by the Complete Street Address, City, State, and Zip Code where the Alternate Health Care Agent resides and may be physically located. 5 – Execute This Paperwork Through The Principal’s Signature
5 – Execute This Paperwork Through The Principal’s Signature
The Principal who is issuing this paperwork to designate the Health Care Agent must provide a notarized signature. To begin, he or she will need to enter the Calendar Day (1,2,3, etc.), Calendar Month, and Calendar Year when the Principal’s Signature occurs across the three blank spaces in the statement “Signed this…” Next, the Principal will need to sign his or her Name on the blank space labeled “Signature of Principal.”
Next, the Principal will need to sign his or her Name on the blank space labeled “Signature of Principal.” Directly below the Signature, the Principal must Print his or her Name.
Directly below the Signature, the Principal must Print his or her Name.  Finally, the Principal’s Address of Residence should be supplied using the next two lines.
Finally, the Principal’s Address of Residence should be supplied using the next two lines.  The Notary Public observing the act of Principal Signing will also have an area that must be attended to. Only the Notary Public can satisfy the requirements in the area below the statement “This Power of Attorney must be witnessed by two persons or notarized.”
The Notary Public observing the act of Principal Signing will also have an area that must be attended to. Only the Notary Public can satisfy the requirements in the area below the statement “This Power of Attorney must be witnessed by two persons or notarized.” The last area to be focused on may only be satisfied by the Witnesses who have seen the Principal Signing at the time of Principal Signing. Each Witness must locate the statement beginning with “By signing this form I declare…” Below this statement will be two defined columns. One Witness should fill out one of these columns with his or her Signature, Printed Name, Street Address, City, State, and Zip Code.
The last area to be focused on may only be satisfied by the Witnesses who have seen the Principal Signing at the time of Principal Signing. Each Witness must locate the statement beginning with “By signing this form I declare…” Below this statement will be two defined columns. One Witness should fill out one of these columns with his or her Signature, Printed Name, Street Address, City, State, and Zip Code.