Updated October 22, 2023
A Hawaii advance health care directive allows a person to select a medical care agent to handle their health treatment wishes. It gives instructions to medical staff on how to be treated in the event of being incapacitated permanently. For these reasons, advance directives are common for the elderly or any individual seeking a health care plan.
Advance Directive Includes
- Part 1. Individual Instructions for Health Care
- Part 2. Health Care Power of Attorney Agent’s Authority and Obligation
Table of Contents |
Laws
Statute – Chapter 327E (Uniform Health Care Decisions)
Signing Requirements (§ 327E-3(b)) – Two (2) witnesses or a notary public. Persons authorized to act as witnesses are expressly defined in § 327E-3(c)(d).
State Definition (§ 327E-2) – “Advance health-care directive” means an individual instruction or a power of attorney for health care.
Versions (4)

Download: PDF

Download: PDF

Download: PDF

Download: PDF
How to Write
Download: PDF
Hawaii Principal Identity
(1) Document Date. The directive being composed must be dated. Record the date this paperwork is completed or put in effect.
(2) Your Name. Establish this paperwork as your directive by identifying yourself as the Hawaii Principal or Hawaii Declarant setting treatment instructions for the review of future attending Physicians in this state.
(3) Full Address.
Part 1: Individual Instructions For Health Care
(4) Choice To Prolong Or Not To Prolong Life. If you are incapacitated by being permanently unconscious, stricken with a neurological condition that severely impairs your ability to comprehend or communicate, or are in the final stages of a fatal condition then some treatment decisions would be discussed beginning with your preference in life-support or life-prolonging equipment and techniques. Use your initials as an instrument to adopt one of the statements in Choice A as your directive. In this way, you can inform Hawaii Physicians on whether you request all life-prolonging techniques available employed when necessary to keep you alive or you can inform Hawaii Physicians that you do not wish life-prolonging equipment and techniques applied when incapacitated and/or near death.
(5) Artificial Nutrition And Hydration (Food And Fluids) By Tube. If you are unable to care for yourself when incapacitated, near death, or unable to communicate then you run the risk of being unable to eat or drink on your own. If the risk of choking exists for hand feeding or assisted feeding then Hawaii Medical Staff will seek your consent to deliver food and water intravenously or through a tube. Use the next statement to inform future Reviewers on whether you will accept food and water through a tube or intravenously or if you refuse food and water delivered this way even when running a high risk of starvation/dehydration.
(6) Relief From Pain. If suffering because of an end-of-life event or as a result of severe incapacitation (i.e. neurological damage), then Hawaii Physicians shall attempt to gain your consent to pain management. If you wish to be kept as pain-free as legally allowed then initial the appropriate choice in Statement C. Otherwise, to deny pain management when in such a condition, provide your initials where requested.
(7) Ethical, Religious, Or Spiritual Instructions. As the Hawaii Declarant or Principal issuing this directive, you may present the name and contact information for the church, spiritual organization, or religious group that you wish informed of your incapacitation or life-threatening medical condition. If appropriate, you may also include any pertinent end-of-life instructions for your spiritual needs.
(8) Hospice Care. When suffering an end-of-life event many opt for hospice care for support. Select the “Yes” or “No” box to indicate if, as the Hawaii Declarant or Principal, you wish to receive hospice care or choose to deny it.
(9) Primary Care Physician. The full name and telephone number of the Primary Physician you wish contacted for information regarding your medical condition should be dispensed to this document for the benefit of your future attending Hawaii Physician’s benefit.

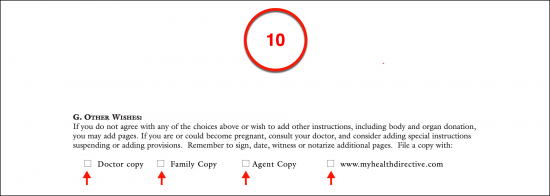
(10) Other Wishes. Any other instructions regarding medical care and treatment choices you wish Hawaii Physicians to be aware of or follow should you be rendered incognizant, with an incurable, painful, and permanent neurological impairment, and/or permanently unconscious can be presented as an attachment to this document so long as such attachment is present when this paperwork is signed and notarized (or witnessed). A copy of all such documents may be filed with additional Parties. Select every Party that shall hold a copy of your medical directives from the list provided.
Part 2 Health Care Power Of Attorney Agent’s Authority
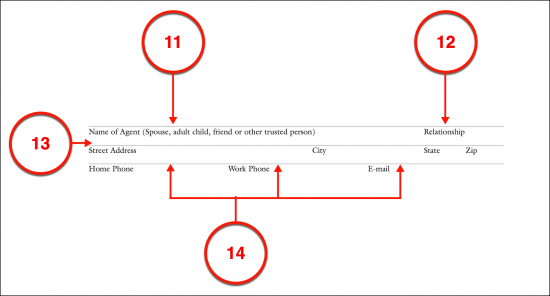
(11) Name Of Agent. This directive provides the option to appoint a Health Care Attorney-in-Fact or Agent who is approved to consult with Hawaii Doctors and determine medical treatment at a time when you are permanently incapacitated or unconscious. This Party can only act in such a capacity if his or her name is attached to this role.
(12) Agent Relationship. The Hawaii Health Care Attorney-in-Fact or Agent’s relationship with you (the Principal or Declarant) should be documented.
(13) Full Address.
(14) Direct Agent Contact. The Hawaii Health Care Attorney-in-Fact’s current telephone numbers (i.e. home, work, cell, etc.) should be supplied along with his or her e-mail address.
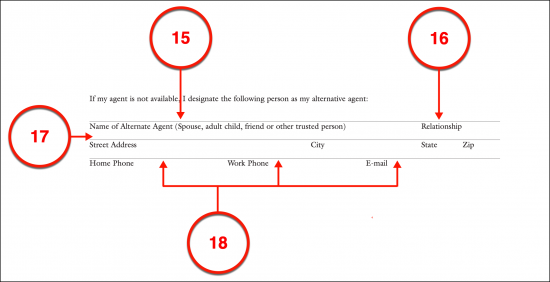
(15) Name Of Alternate Agent. Hawaii Doctors might not be able to use the Health Care Attorney-in-Fact or Agent when needed which would leave you without anyone to discuss your preferred treatment consents and inform them of procedures you would refuse. This may be because he or she is traveling and unavailable, has been revoked, or cannot uphold your directives. In any case, to make sure that you have an Agent to work with Hawaii Physicians regarding your treatment, you can set up an Alternate Agent to take over this role. Produce this Party’s name so that he or she can be approached to act as your Attorney-in-Fact when your first choice will not or cannot act with your medical authority. Be advised the Alternate Hawaii Health Care Agent will not be granted any of your decision-making powers unless your initial choice of Agent does not fill the role.
(16) Relationship.
(17) Full Address.
(18) Alternate Agent Contact Information.
Health Care Agent And Decision Making
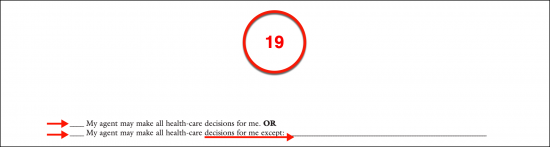
(19) Level Of Authority. Your Health Care Agent (or Attorney-in-Fact) can be given the authority to act to the fullest extent this role allows in the State of Hawaii or you may limit his or her powers by placing limits and documenting specific instructions. Produce your initials to the statement that best applies to this status. Notice that if you wish to place limitations or instructions, a predetermined area has been set aside where you may report them or cite an attachment with these medical instructions and Agent limitations by name.
(20) Time Of Effect. The time when your Hawaii Health Care Agent or Attorney-in-Fact is given the authority to speak for your medical decisions can be set to the first day that you are diagnosed as incapacitated and unable to communicate or the moment your witnessed or notarized signature is produced to this directive. One of two statements allowing this determination to be applied should be approved by your initials.
Your Name And Signature
(21) Print Your Name. Once you have decided whether your signature will be observed for authenticity by two Witnesses or one Notary Public, gather with the appropriate Party and the directive just completed. Begin the execution of this form by printing your full name.
(22) Your Signature. Sign your name to claim the completed directive as your own. As the Hawaii Declarant or Principal issuing this directive, your signature should be easily verifiable in the future. Thus, your signature should be dispensed before either two Witnesses or one Notary Public.
(23) Date. Record the date that you have signed your name then give this signed document to the Party that has watched your signing.
Witness Testimony Option
(24) Witness # 1. The first Witness to verify your act of signing must print his or her name, provide a dated signature, and record his or her address.
(25) Witness # 2. The second Witness in attendance should take control of this paperwork once the first Witness has completed his or her signature testimony. Witness #2 must authenticate your signing by printing and signing his or her name, documenting the current date, and presenting his or her address.
Notary Public Option
(26) Notarization. If you have decided to sign this document as the Hawaii Principal before a Notary Public, then he or she will notarize your signature in the area provided using his or her credentials.
Related Forms
 Durable (Financial) Power of Attorney
Durable (Financial) Power of Attorney
Download: PDF, MS Word, OpenDocument
Download: PDF, MS Word, OpenDocument