Updated August 08, 2023
An Arizona medical power of attorney is a document that allows a family member or spouse to handle the medical needs of another person. The power of attorney is written by a principal in case they cannot speak to the medical staff themself. This is common due to Dementia, Alzheimer’s Disease, or resulting from recent surgery. A medical power of attorney can be canceled at any time by the principal completing a Revocation Form.
How to Write
Download: PDF
1 – Open The Form Once The Reference Information Has Been Gathered
Once the Principal has gathered and organized any additional or supplemental paperwork, open the form here on this page (below the image). Save this form for safekeeping. You may work on-screen with the appropriate software.
2 – The Principal of this Authority will need to be identified in the first section by entering the requested information
Several labeled lines have been provided for this purpose. Enter the Name of the Principal on the “My Name” line. Then, on the “My Address” line, enter the Principal’s Address.
On the right will be a column of lines requesting the principal’s Age, Date of Birth, and Telephone Number. Use the lines labeled “My Age,” “My Date ofBirth,” and “My Telephone Number” to report this information.
3 – Declare The Identity Of The Agent And Provide Contact Information
The second section will also have several blank lines requesting information, however, this will refer to the Agent or Surrogate. That is, the entity who will have Medical Decision Making Powers regarding the Principal’s Health. First, use the “Name” and “Address” lines to declare the Full Name of the Surrogate Agent and record the Surrogate Agent’s Address.
The column of blank lines on the right hand side, in Section 2, must have Surrogate Agent’s Contact Information. Enter the Surrogate Agent’s Home Telephone Number, Work Telephone Number, and Cell Phone Number on the blank lines labeled “Home Phone,” “Work Phone,” and “Cell Phone”
This section will also allow for an Alternate Representative to be elected and reported by the Principal. This party will step up to the Surrogate Agent’s responsibilities if he or she cannot, will not, or is no longer allowed to wield Principal Medical Decision Making Powers. Below the statement starting with “I choose the following person to act…,” utilize the blank lines labeled “Name,” “Address,” “Home Phone,” “Work Phone,” and “Cell Phone” to document the Alternate Representative’s Identity, Home Address, and Contact Information.
4 – Read The Third Item, Then Document The Principal’s Limitations
The Third Section will define some of the actions and decisions a Surrogate Agent may affect as a result of this document. Make sure the Principal understands these statements and all relatable statutes. Once this task is complete, the Principal should document any limitations, restrictions, conditions, or specifications in the space below the statement starting with “I do not want my representative…” in Section 4.
5 – The Principal’s Autopsy Preferences
Item 5 provides a section where the Principal may divulge his or her preferences in terms of having an autopsy after death. Locate the heading “5. My specific desires about autopsy.” Three statements with blank lines will be provided beneath “Note” box. If the Principal does not consent to an Autopsy, he or she should initial or mark the blank line preceding the words “Upon my death I DO NOT consent…” If the Principal does not object to an Autopsy, he or she should mark or initial the blank line preceding the second statement.
If the Principal does not object to an Autopsy, he or she should mark or initial the blank line preceding the second statement.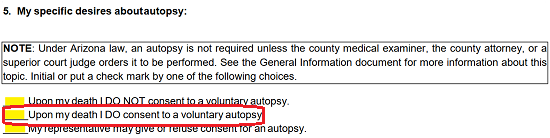
The Principal may elect to give the Surrogate Agent/Representative the power to make this decision. If so, then he or she should mark or initial the third statement.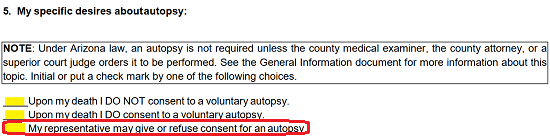
6 – The Principal Anatomical Gift Preferences
Section 6, “My specific desires about organ donation…,” presents two simple statements. If the Principal does not wish to make any Anatomical Gifts (i.e. Organ Donation), he or she should initial or mark Choice A. If the Principal does wish to make Anatomical Gifts, he or she should mark Choice “B,” then proceed to the questions below to further define the nature of the Anatomical Gifts to be made.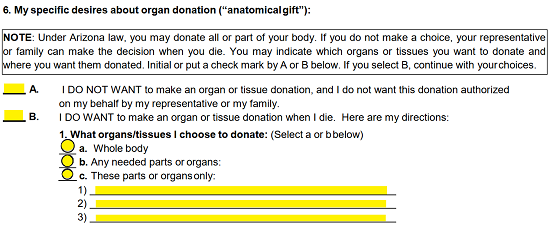
If the Principal has indicated that he or she wishes to make Anatomical Gifts, then Item 1 will allow for some specifications to be made. The Principal may choose to donate his or her Whole Body by filling in the “a” bubble, Any Needed Parts/Organs by filling in the “b” bubble, or specific parts/organs by filling in the “c” bubble. Note: If selecting “c,” the specific parts/organs must be defined on the numbered lines below this choice.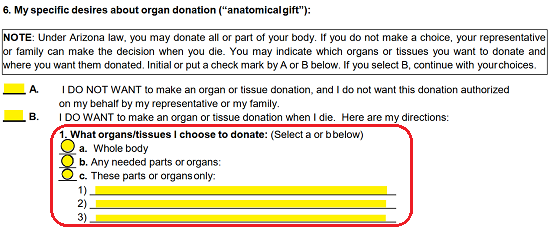
The next item will allow the Principal to quickly name the Purpose Anatomical Donations may be made (if any). If the principal authorizes Anatomical Gifts be made for any legal purpose, the first bubble must be marked or filled in. If the Principal will only approve of Anatomical Gifts for Transplants or Therapeutic Purposes, the “b” bubble will need to be filled in. If the Principal will only allow Anatomical Gifts for Research Purposes, the “d” bubble should be filled in. The Principal may have other specific Purposes for Anatomical Gifts. If so, select “d,” then enter the Approved Purpose on the blank line.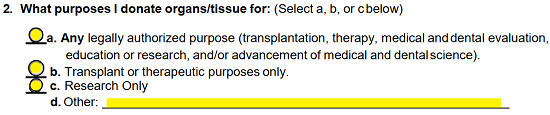
The Principal may also have preferences as to where Anatomical Gifts can be made. In Item 3, the Principal may name the Organizations or Individuals who his or her Anatomical Gifts may be made. Fill in the “a” bubble if the Principal has already signed a written agreement with an individual or institution recipient and document the Identity of this entity on the blank lines provided. If the Principal has no such agreement but wishes his or her Anatomical Gifts be made to a specific entity, then mark the “b” bubble and record the Entity Name on the blank line provided. The Principal may choose to allow the Surrogate or Representative to make this decision by filling in the “c” bubble.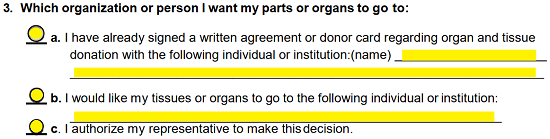
7 – The Option To Define Disposition
If the Principal has preferences or instructions regarding “Funeral and Burial Disposition” arrangements, they may be made in Section 7. This section will contain a list of items with a blank line preceding each one. The Principal should initial or mark the statement(s).
If the Principal wishes his or her body to be buried, then he or she should initial the first statement.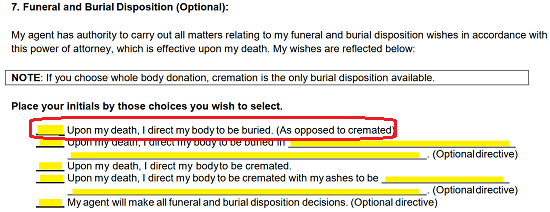
If the Principal wishes his or her body to be buried and intends for specific instructions to be followed, then he or she should initial the second statement. There will be a blank line in the second statement where the Principal must indicate what the special instructions are.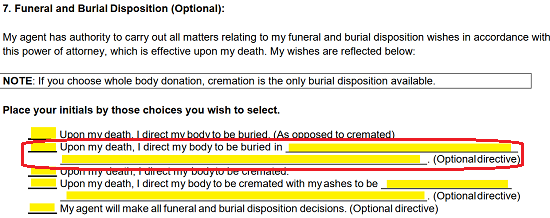
The Principal also has the option of the directing for a cremation. If so, then he or she should initial the third statement.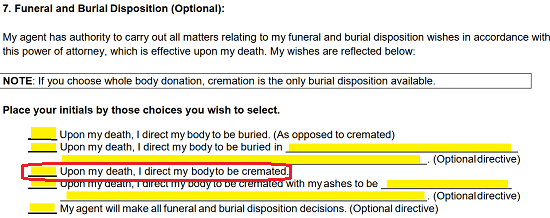
Should the Principal prefer a cremation and has instructions regarding this, then he or she should initial the fourth statement.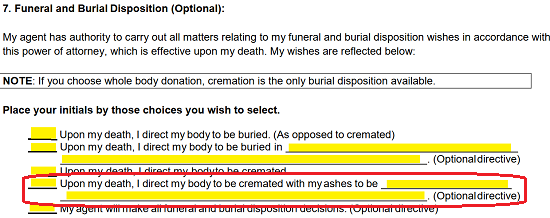
The Principal may opt to have the Surrogate Agent make such decisions. If so, then he or she should initial the fifth statement. This will empower the Agent to make funeral/burial/cremation decisions on behalf of the Principal.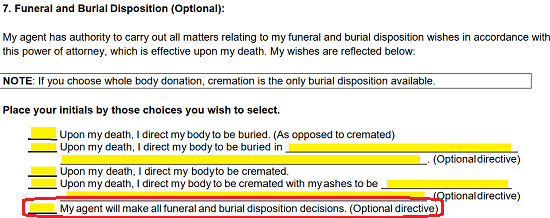
8 – A Principal’s Living Will Should Be Reported In This Document
If the Principal has signed a Living Will this should be attached to this form and indicated. Locate Section 8 titled “About A Living Will.” If the Principal has signed and attached a Living Will, he or she should initial Choice “A,” then attach the full and completed Living Will. If this is not the case, the Principal must indicate he or she has not signed a Living Will and thus, no such document is attached by initialing Choice “B.”
9 – The Principal’s Resuscitation Instructions
If the Principal has signed a Prehospital Medical Care Directive or a Do Not Resuscitate Directive on Paper with Orang background, then he or she should attach this document and initial Choice “A.” If not, then he or she should initial Choice “B.”
10 – The HIPAA Waiver
If the Principal authorizes the Agent to have the same rights regarding disclosure and use of the Principal’s Health/Medical information according to the Health Insurance Portability and Accountability Act (HIPAA) of 1996, then he or she should initial the blank line next to the statement in Section 10. If not, then he or she should leave this statement unmarked.
11 – The Principal’s Clear Approval And Verification
Find the heading “Signature or Verification.” Item “A” will require the Principal to sign the blank line labeled “My Signature.” When done, the Principal should enter the Date he or she signed this document on the blank line labeled “Date.”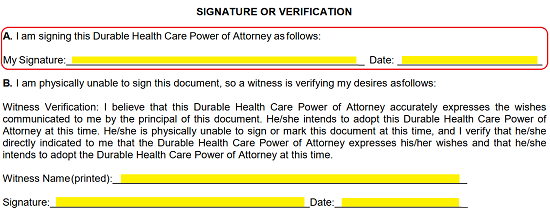
Item B has been provided in the case where the Principal is unable to sign this document. Here, a Witness who has received instructions verifying this document’s directives may Sign to validate its authenticity. If this is the case, such a Witness should read the Item B Statement, then Print his or her Name on the “Witness Name” line and sign his or her Name on the “Signature” line. The Date of this Signature should be entered by the Signature Party on the blank line following the word “Date.”
12 – Second Party Verification
This document’s signing may be verified through one Adult Witness or a Notary Public. Each will have a distinct area beneath the heading “Signature of Witness or Notary Public.” If this document’s signing will be verified by a Witness, the Witness will need to Print and Sign his or her Name. The Date of Signature must be reported on the “Date” line and the Witness’ Address should be entered using the blank lines next to “Address.”
If this document’s signing will be validated by a Notary Public, the Notary Public will need to fill in the page beginning with the words “Notary Public.” This entity is the only one who may fill in any information on this page and stamp it with a valid notary seal.
13 – Physician Statement
If the Principal has fully discussed the Directives he or she has supplied in this form with a Physician, it may be wise to have the Physician sign the Physician Statement as this will verify the Principal’s understanding of the powers in this document (amongst other things). There will be several blank lines beneath the heading “Statement That You Have Discussed Your Health Care Choices For The Future With Your Physician.” The Physician who can agree with this statement will need to Print his or her Name on the “Doctor Name” line. Below this, he or she should Sign and Date the blank lines provided. Finally, the Doctor should supply his or her Address on the “Address” lines.