Updated August 08, 2023
An Arkansas medical power of attorney grants a trusted friend or relative of the principal the power to make medical decisions on their behalf should the principal not have the capacity to do so. This is a useful document to have in place before you have surgery or some other scheduled medical procedure where you will be under anesthesia. In addition, it is something that will be helpful in the event of an unscheduled trip to the hospital.
How to Write
Download: PDF
1 – Save The File On This Page To delegate Health Care Power To An Agent In The State Of Arkansas
The paperwork available on this page can be used to name one or more individuals with the health care powers required to represent him or her when incapacitated and/or unable to communicate with medical staff. This file is available as a pdf through the link above or the button under the image. You may access it using a PDF editor on your computer or you may print it using your browser then fill it out by hand.
2 – Prepare This Document With Some Basic Information
Once you are ready to report the directives of the Principal who intends to appoint a Health Care Agent by executing this document. Begin by reporting your name, if you are the Principal, on the blank line below the title. This space must record the full name of the individual naming an Attorney-in-Fact.  Next, produce the full name of the individual who shall take up the role of the Health Care Agent on the first blank line in the first statement. This individual will act as a representative of the Principal but only when the Principal is incapacitated or otherwise unable to communicate (as per the Arkansas Health Care Decisions Act).
Next, produce the full name of the individual who shall take up the role of the Health Care Agent on the first blank line in the first statement. This individual will act as a representative of the Principal but only when the Principal is incapacitated or otherwise unable to communicate (as per the Arkansas Health Care Decisions Act).  Naturally, a method to quickly reach the Health Care Agent will need to be included with this paperwork. To this end, provide the Health Care Agent’s telephone number on the blank space between the words “…Whose Phone Number Is” and the term “To Make Decisions…”
Naturally, a method to quickly reach the Health Care Agent will need to be included with this paperwork. To this end, provide the Health Care Agent’s telephone number on the blank space between the words “…Whose Phone Number Is” and the term “To Make Decisions…” 
3 – Review And Approve The Principal Actions The Attorney-in-Fact May Take
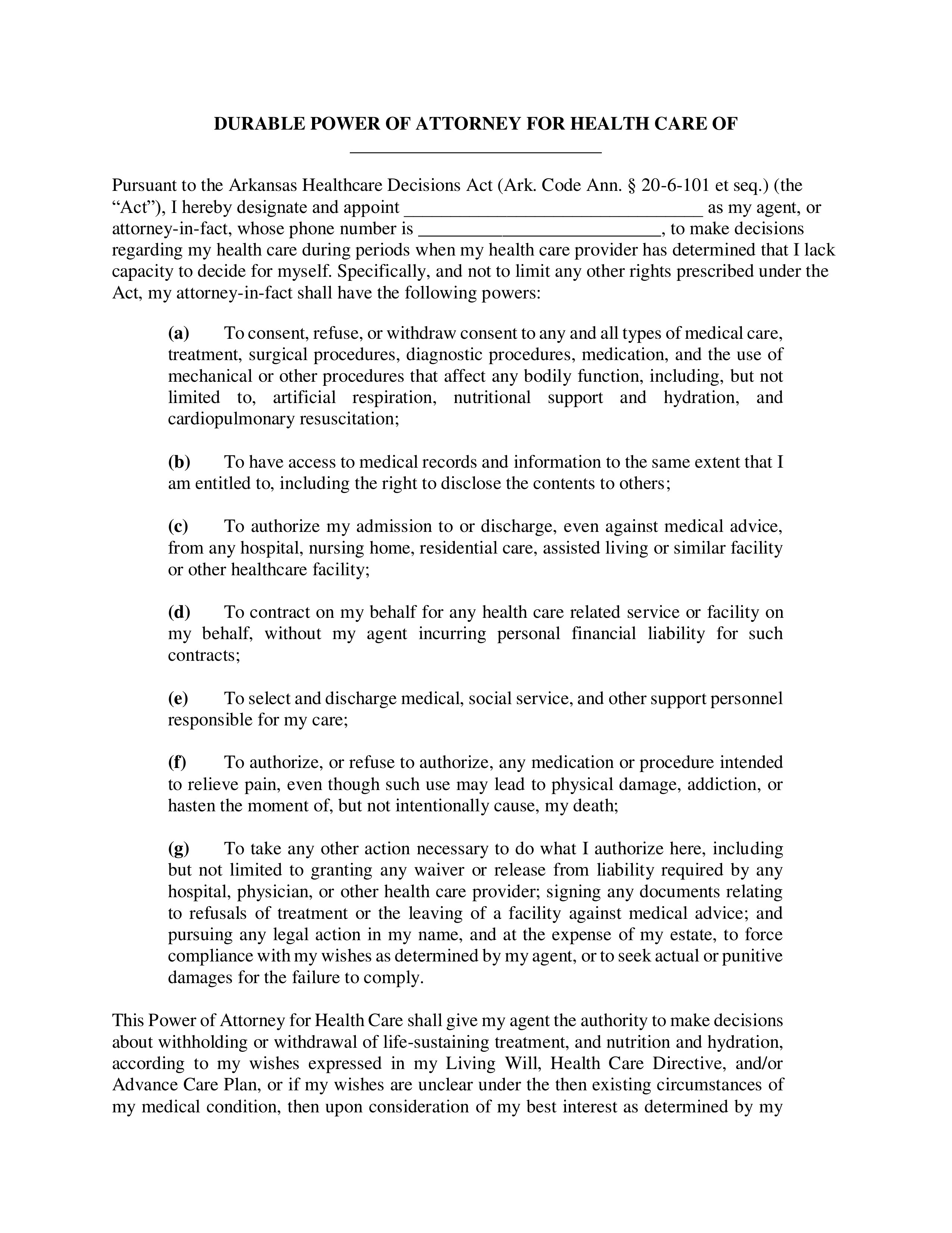
A list of actions the Attorney-in-Fact may take on behalf of the Principal is presented after this introduction. It will be up to you, the Principal, to review each statement on this list. Each item on this list delivers a definition to the Attorney-in-Fact’s healthcare powers when representing the Principal. If you do not wish the Attorney-in-Fact to have the authority to take one or more of these actions when representing, you then you must delete or cross out that statement. The example below will illustrate a Principal who authorizes the Attorney-in-Fact to take every action on this list except for those in “(C).” The Principal in this example does not authorize the Attorney-in-Fact’s right “To Select And Discharge Medical, Social Service, And Other Support Personnel” on his or her behalf. Thus, to restrict the Attorney-in-Fact’s powers of representation, the Principal here has crossed out this item. See example. 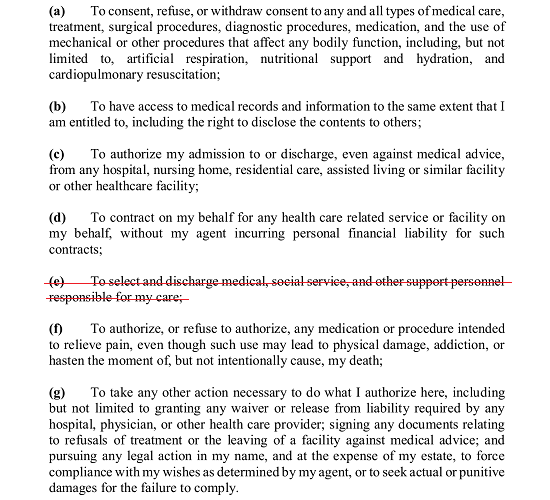 If you do not wish the Attorney-in-Fact to have the authority “To Consent, Refuse, Or Withdraw Consent To Any And All Types Of Medical Care” on your behalf then cross out statement “(A)”
If you do not wish the Attorney-in-Fact to have the authority “To Consent, Refuse, Or Withdraw Consent To Any And All Types Of Medical Care” on your behalf then cross out statement “(A)”  Statement “(B)” will give the Attorney-in-Fact the right to access your medical records and information with the same authority you carry. If you do not wish the Attorney-in-Fact to have this type of principal power, you must cross out or delete this statement.
Statement “(B)” will give the Attorney-in-Fact the right to access your medical records and information with the same authority you carry. If you do not wish the Attorney-in-Fact to have this type of principal power, you must cross out or delete this statement. ![]() The third statement empowers the Attorney-in-Fact to perform actions such as deciding upon your admission, discharge, or length of stay with a medical facility. If you do not wish to grant your Attorney-in-Fact the right to make such decisions then, remove or strike through statement “(C).”
The third statement empowers the Attorney-in-Fact to perform actions such as deciding upon your admission, discharge, or length of stay with a medical facility. If you do not wish to grant your Attorney-in-Fact the right to make such decisions then, remove or strike through statement “(C).”  If you intend to grant the Attorney-in-Fact the right to represent you with the authority to contract health care professionals, services, or facilities on your behalf then leave statement “(D)” intact. To forbid the Attorney-in-Fact from taking part in such actions on your behalf, then delete or cross out this statement.
If you intend to grant the Attorney-in-Fact the right to represent you with the authority to contract health care professionals, services, or facilities on your behalf then leave statement “(D)” intact. To forbid the Attorney-in-Fact from taking part in such actions on your behalf, then delete or cross out this statement.
 The Attorney-in-Fact will have the principal power to “To Select And Discharge Medical, Social Service, And Other Support Personnel” using your name through the language in statement “(E).” To deliver such principal power, leave this statement unaltered. Cross out, delete, or remove this statement to restrict the Attorney-in-Fact from such actions.
The Attorney-in-Fact will have the principal power to “To Select And Discharge Medical, Social Service, And Other Support Personnel” using your name through the language in statement “(E).” To deliver such principal power, leave this statement unaltered. Cross out, delete, or remove this statement to restrict the Attorney-in-Fact from such actions. ![]() The language in statement “(F)” allows your Attorney-in-Fact to have the same power of authorization over pain management treatments that you do. You may either leave this statement in or cross it out.
The language in statement “(F)” allows your Attorney-in-Fact to have the same power of authorization over pain management treatments that you do. You may either leave this statement in or cross it out.  Statement “(G)” will assume you wish to grant your Attorney-in-Fact a broad scope of principal power regarding your health care and the results of your incapacitation. Read this statement thoroughly. You may leave it intact to authorize the Attorney-in-Fact to take these actions on your behalf, strike through any of the described actions to restrict the Attorney-in-Fact’s ability to perform them, or simply remove/strike-through this statement to forbid the Attorney-in-Fact from such a wide range of principal power.
Statement “(G)” will assume you wish to grant your Attorney-in-Fact a broad scope of principal power regarding your health care and the results of your incapacitation. Read this statement thoroughly. You may leave it intact to authorize the Attorney-in-Fact to take these actions on your behalf, strike through any of the described actions to restrict the Attorney-in-Fact’s ability to perform them, or simply remove/strike-through this statement to forbid the Attorney-in-Fact from such a wide range of principal power. 
4 – Additional Parties May Be Named As A Precaution Through This Paperwork
The last statement in this document will give you the opportunity to name a successor to the principal power you have granted the Attorney-in-Fact, should he or she not wish to represent you, is ineligible to use principal power, or cannot act in this role for one reason or another. Rather, then risk being unprotected while a new Attorney-in-Fact document is delivered, you can simply name a Successor or Alternate Attorney-in-Fact to step in if necessary. To name such an entity, report the original Attorney-in-Fact’s full name on the first blank space and the Successor Attorney-in-Fact’s name on the second blank space.  An optional statement has been included in blue text. This is not necessarily a statement of power being delivered but a nomination should a Court-Appointed Guardian or Conservator is required. This statement will not solidify this role for anyone you name here however, the courts will take it into consideration if it is submitted in a timely manner. To nominate such an individual, replace the labels “FULL NAME,” “FULL ADDRESS,” and “Phone Number” with the name, address, and telephone number of your nomination.
An optional statement has been included in blue text. This is not necessarily a statement of power being delivered but a nomination should a Court-Appointed Guardian or Conservator is required. This statement will not solidify this role for anyone you name here however, the courts will take it into consideration if it is submitted in a timely manner. To nominate such an individual, replace the labels “FULL NAME,” “FULL ADDRESS,” and “Phone Number” with the name, address, and telephone number of your nomination. 
5 – A Witnessed And Notarized Signature From The Principal Is Required To Correctly Execute This Directive
Locate the statement just above the “Signature” line. Use the three spaces following the word “Signed” to report the current calendar date the day you sign this document.  Sign your name on the “Signature” line as soon as you have recorded the current date before two Witnesses and a Notary Public. Surrender this document to one of these parties once you have provided your signature.
Sign your name on the “Signature” line as soon as you have recorded the current date before two Witnesses and a Notary Public. Surrender this document to one of these parties once you have provided your signature.  The following sections are to ensure a proper signature has been supplied. The Preparer of this document or one of the Witnesses must supply the full name of the individual who has just signed his or her name on the blank space following the word “Declarant.
The following sections are to ensure a proper signature has been supplied. The Preparer of this document or one of the Witnesses must supply the full name of the individual who has just signed his or her name on the blank space following the word “Declarant.  Each Witness must read this statement and the numbered statements to the side then print and sign his or her name on the lines labeled “Print Witness Name” and “Signature Of Witness.”
Each Witness must read this statement and the numbered statements to the side then print and sign his or her name on the lines labeled “Print Witness Name” and “Signature Of Witness.”  The next party to control this paperwork will be the Notary Public. He or she will complete the “Acknowledgment” after witnessing the signature parties above then supply his or her seal.
The next party to control this paperwork will be the Notary Public. He or she will complete the “Acknowledgment” after witnessing the signature parties above then supply his or her seal.