Updated January 29, 2024
A Wyoming advance directive is a document used in the case of an emergency to outline a person’s health care instructions if they cannot speak for themselves. It allows an agent to be selected and handle medical decisions on the patient’s behalf and instructions on the preference for health care. The document should be kept in a safe and accessible place in the event of an emergency.
Four (4) Parts
- Power of Attorney for Health Care;
- Instructions for Health Care (living will);
- Donation of Organs; and
- Information about Health Care Providers.
Table of Contents |
Laws
Statutes – Title 35, Chapter 22 (Living Will)
Signing Requirements (§ 35-22-403(b)) – Two (2) witnesses or a notary public.
State Definition (§ 35-22-402(a)(i)) – “Advance health care directive” means an individual instruction or a power of attorney for health care, or both.
Versions (6)
- AARP
- Campbell County Health
- Cheyenne Regional Health
- Ivinson Hospital
- University of Wyoming
- Wyoming Medical Center

Download: PDF

Download: PDF
Download: PDF

Download: PDF

Download: PDF

Download: PDF
How to Write
Download: PDF
Wyoming Advance Health Care Directive
(1) Wyoming Health Care Principal. It is imperative that Wyoming Medical Professionals can easily identify this directive immediately in your files. Therefore, submit your full name to the title page.

Identify This Paperwork
(2) Print Your Full Name. In addition to properly claiming this paperwork, you should indicate when you have attended to each page and initial your approval upon its completion. Record your name to the top of every page along with the requested authorization items.
(3) Today’s Date. Dispense the current calendar date to demonstrate precisely when you have reviewed and authorized the information presented on this page.
(4) Initial That You Have Completed The Page.
Part 1. Power Of Attorney For Health CareArticle 1 Designation Of Agent
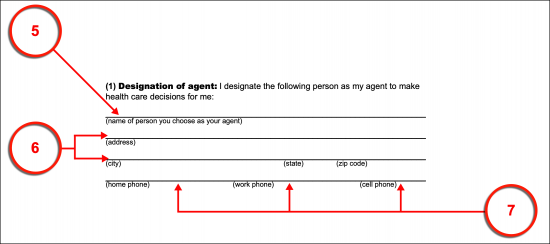
(5) Name Of Person You Choose As Your Agent. Determine who should be appointed to interact with Wyoming Doctors in discussions and decisions over your health care treatment in this state. This Party, known as the Wyoming Health Care Agent, will be considered to know the treatments you authorize. Therefore, he or she will be contacted by Wyoming Physicians to gain your treatment approvals/refusals and instructions. Once you have decided on who should take this responsibility as well as the granted power needed to live up to it, you must document your Wyoming Health Care Agent’s name.
(6) Wyoming Health Care Agent Address.
(7) Contact Home, Work, And Cell Phone Number.
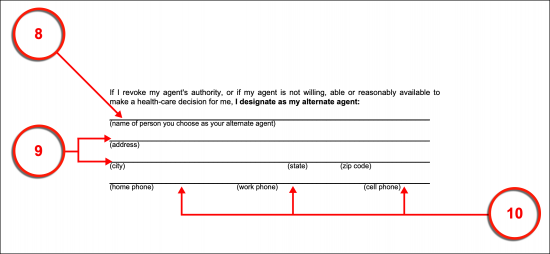
(8) Name Of Person You Choose As Your Alternate Agent. The Party who you expect to serve as your Wyoming Health Care Agent may not be available to do so when needed may have been revoked and disqualified from acting in this capacity at the time or may decline. An Alternate Wyoming Health Care Agent is thus a recommended designation in this form. The Alternate Wyoming Health Care Agent can potentially receive all the granted abilities this document delivers however only if the Party you initially chose does not fulfill the Wyoming Agent’s role and responsibilities (at which time the Alternate Wyoming Agent will take over). This type of precaution can prove invaluable. Take this opportunity to appoint your Alternate Health Care Agent as an Agent in reserve by dispensing his or her full name to this document.
(9) Address Of Wyoming Alternate Agent.
(10) Wyoming Alternate Agent Contact Telephone Numbers. It can be imperative that Wyoming Physicians be able to reach your Alternate Wyoming Health Care Agent immediately, thus provide his or her current phone numbers for contact.
Article 2 Agent’s Authority
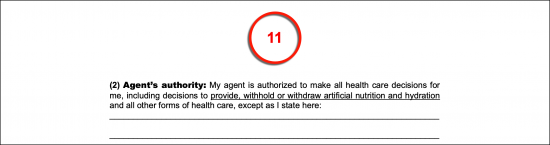
(11) Discuss The Intended Grant Of Decision-Making Power. The limitations that you wish to apply to the Wyoming Health Care Agent’s principal power to make medical decisions over your treatment must be documented. Otherwise, it will be assumed that your Wyoming Health Care Agent will receive the full scope of abilities the State of Wyoming grants to this appointment.
(12) Approve Of The Third Page. Review the information that you provided to the third page after you have completed it. If it reflects your intended directives, then supply your name in print along with the current calendar date and your initials.

Article 3 When Agents Power Becomes Effective
Select Item 13, Item 14, Or Item 15
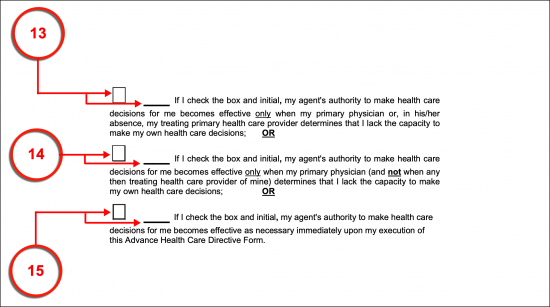
(13) Only Upon Incapacitation Declared By Primary Or Attending Physician. The circumstances by which your Wyoming Health Care Agent is designated with principal authority over your medical decisions must be set. If you only wish to grant the Wyoming Health Care Agent principal upon the prognosis of your incapacitation by the Attending Physician or your Primary Physician, then you must mark the first checkbox and deliver your initials next to it. This means that so long as you are conscious and able to represent yourself, the Wyoming Health Care Agent will not automatically be granted the approval needed to represent you.
(14) Only When Primary Physician Declares Incapacitation. If you have decided that only your Primary Physician may make the declaration that you are incapacitated thus prompting this document to deliver principal power to your Wyoming Health Care Agent, then you must select the second checkbox and dispense your initials to the right. This also means that your Wyoming Health Care Agent will only be able to represent your interests when you are unconscious.
(15) Immediately Upon This Directive’s Execution. If desired, you can set this directive to grant the Wyoming Health Care Agent immediate principal power. This means that as soon as you sign your name, he or she will be able to carry out your health care directives and convey them to Medical Personnel in this state. In this option, you do not have to be incapacitated or unconscious for his or her principal powers to become active. It should be noted that your Wyoming Health Care Agent will not have the ability to override any of the decisions you issue unless you have specifically authorized him or her to do so beforehand (in the previous section).
(16) Fourth Page Confirmation.
Part 2 Instructions For Health Care
Article 5 End-Of-Life Decisions
Select Item 17 Or Item 18
(17) Choice To Prolong Life. Wyoming Physicians will attempt to prolong life whenever possible however, a Patient in the end-stages of a fatal illness, injured where death is inevitable, or in a permanent vegetative state may require invasive life-support technology such as intubation, dialysis, which will result in pain or even permanent (additional) injury, or surgical implants to continue living. Such procedures are best administered with the full authorization of the Patient. If you would like to instruct Wyoming Physicians to keep you alive as long as medically possible regardless of the procedure or medication required then select and initial the first statement in Article 5.
(18) Choice Not To Prolong Life. While Wyoming Physicians will seek to prolong life, they will also respect a Patient’s wishes if he or she prefers a natural death as opposed to seeking to prolong life unnaturally. If you prefer to inform Wyoming Physicians that life-sustaining procedures, surgeries, and medications should be withheld when death is close and such maneuvers are the only way to continue living, then select and initial the statement provided.
Article 6 Artificial Nutrition And Hydration
Choose Item 19 Or Item 20
(19) Requiring Artificial Nutrition Regardless Of Condition. When a Wyoming Physician declares you as incapacitated and unable to pass on your treatment preferences, you will be unconscious (for life), enduring a terminal condition that results in your death without life-sustaining treatment, or have a fatal medical condition that shall result in death whether you are given life-support or not. In most cases, you will lose your ability to eat and/or absorb nutrition during this time so Wyoming Physicians will seek to deliver nutrition directly to your body. This can only be accomplished through your approval. Ensure that the approval to be given artificial nutrition is received by Wyoming Medical Personnel even if your Agent cannot be found by selecting the first checkbox in Article 6 and initialing your approval.
(20) Refusing Artificial Nutrition Regardless Of Condition. To issue your decision in refusing or denying artificial nutrition even if it will result in death from malnutrition, you must choose and initial the second directive statement.
Select Item 21 Or Item 22
(21) Authorization For Artificial Hydration Regardless Of Condition. A similar decision must be made for Wyoming Medical Professionals seeking to prevent your death from dehydration. If you are no longer able to intake water (liquid or frozen) then you will become dehydrated. If this condition is allowed to persist, then dehydration will result in death. You can inform all Wyoming Health Care Providers reviewing this document that you request as well as authorize artificial hydration delivered to your system whenever needed by marking the third statement’s checkbox and authorizing this choice with your initials.
(22) Denial For Artificial Hydration Regardless Of Condition. If you intend to prevent Wyoming Physicians from administering artificial hydration whether it results in your death or not, then select the final statement. This also requires your initials to demonstrate your intent.
(23) Fifth Page Authorization. Demonstrate your approval for this page once it has been completed with your printed name, the current date, and your initials.

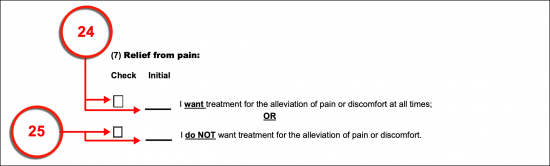
Article 7 Relief From Pain
Select Item 24 Or Item 25
(24) Treatment For The Alleviation Of Pain Directive. Some medical conditions that leave you incapacitated and/or rob you of the ability to communicate can create a nearly intolerable amount of pain. Regardless of whether you have approved or denied artificial nutrition, as the Wyoming Principal, you can request that Physicians monitor your pain and discomfort levels then attempt to provide relief. To deliver this order mark the appropriate checkbox in Article 7 and initial the corresponding blank line.
(25) Refusal Of Treatment For The Alleviation Of Pain. To inform Wyoming Doctors that you do not want pain management utilized to keep you pain-free then check or mark the second checkbox of Article 7 and provide your initials.
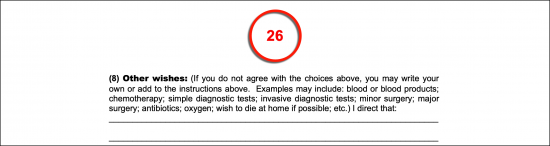
Article 8 Other Wishes
(26) Definitive Treatment Instructions. The nutrition, hydration, and pain management directives above can be issued as is or you may add provisions to these statements. For instance, you may have indicated that you wish artificial nutrition denied but this may be true only for certain medical events that occur or you may wish to approve of artificial techniques for only a limited trial period. Discuss and list every treatment preference you have as your “Other Wishes.”
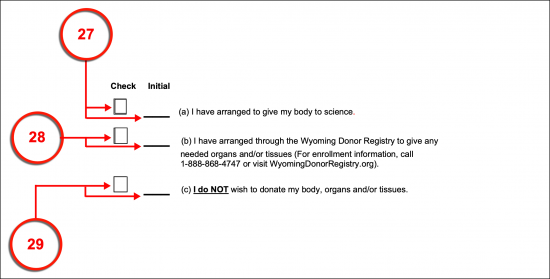
Part 3 Donation Of Organs And Tissues Upon Death
Article 9 Upon Death
(27) Anatomical Donation To Science. This directive can be used to solidify your intent to give your body to science upon death. To issue this declaration choose appropriate chekbox then submit your initials of approval to Statement A.
(28) Official Wyoming Organ Donor. Select Statement B if you have already made arrangements with the Wyoming Donor Registry.
(29) Refraining From Organ Donation. If you do not intend to authorize an anatomical gift of any kind, then you must document this decision by selecting Statement C and dispensing your initials.
(30) Page Six Approval.

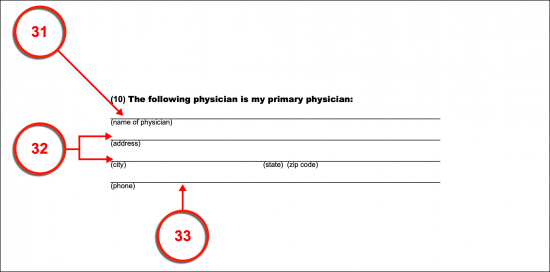
Part 4 Information About My Health Care Provider
Article 10 Primary Physician
(31) Name Of Physician. If you are hospitalized in a Facility that is not familiar with your medical condition and directives, then it will be very useful to attending Wyoming Physicians to have the information needed to contact your Primary Physician. Submit his or her full name and suffix (i.e., M.D.) for review then proceed with a record of his or her address and phone numbers.
(32) Address Of Primary Physician.
(33) Primary Physician Telephone Information.
(34) Name Of Health Care Institution/Hospice. If you regularly record care at a Health Care Facility other than the one treating you while incapacitated, then attending Wyoming Physicians should be given the means to contact this Facility regarding your medical status.
(35) Address And Phone Number Of Primary Institution/Hospice.
Signature Of Wyoming Principal
(36) Print Your Name.
(37) Sign Your Name. Your witnessed or notarized signature is mandatory for this document to be executed properly. Supply this item once you have completed an adequate review of the choices and statements you have provided above.
(38) Signature Date. Document the current date to indicate to Wyoming Physicians reviewing this paperwork as to when you have signed and executed your medical directives for this state.
(39) Address.
Signatures Of Witnesses Or Notary Public
First Witness
(40) First Wyoming Witness Signature. The First Wyoming WItness to control this document after you have executed it must review the confirmation statement regarding your provided signature by attending to the section below it. This requires that the First Witness print his or her name and address then sign and date this area.
Second Witness
(41) Second Wyoming Witness Signature. If you have utilized two Witnesses to confirm your signature as validly produced, then the remaining Witness must complete the Second Witness’s signature area upon his or her agreement to the declaration made regarding your signature. Therefore, the Second Witness should print his or her name, print his or her address, then provide his or her signature and the current calendar date.
Notary Public
(42) Notary Public. A registered Notary Public can be used instead of two Witnesses or with two Witnesses to provide the verification needed to show your signature is both authentic and produced with your awareness. This notarization process will be demonstrated in the final area of this directive and can only be completed by the Notary Public serving the Wyoming Principal’s signing.
Related Forms
 Durable (Financial) Power of Attorney
Durable (Financial) Power of Attorney
Download: PDF, MS Word, OpenDocument

Download: PDF, MS Word, OpenDocument